Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Dębska-Kozłowska2021 Article WhereAreWeIn2021WithHeartFailuДокумент12 страницDębska-Kozłowska2021 Article WhereAreWeIn2021WithHeartFailuSyifa Mahmud Syukran AkbarОценок пока нет
- Lampiran - Moderators of Treatment Efficacy in Individualized Metacognitive Training Metacognitive Training For Psychosis (MCT-) 2020Документ8 страницLampiran - Moderators of Treatment Efficacy in Individualized Metacognitive Training Metacognitive Training For Psychosis (MCT-) 2020Syifa Mahmud Syukran AkbarОценок пока нет
- Heart Failure: Yos Akbar IrmansyahДокумент49 страницHeart Failure: Yos Akbar IrmansyahSyifa Mahmud Syukran AkbarОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- HF DeaДокумент53 страницыHF DeaSyifa Mahmud Syukran AkbarОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Heart Failure & CardiometabolicДокумент99 страницHeart Failure & CardiometabolicSyifa Mahmud Syukran AkbarОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Optimis Gagal Jantung - BIKOДокумент55 страницOptimis Gagal Jantung - BIKOSyifa Mahmud Syukran AkbarОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Overview of Congenital Heart Disease-James YipДокумент1 страницаOverview of Congenital Heart Disease-James YipSyifa Mahmud Syukran AkbarОценок пока нет
- Conti 1991 Clinical - CardiologyДокумент6 страницConti 1991 Clinical - CardiologySyifa Mahmud Syukran AkbarОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Song Et Al 2007 Thyroid HormonesДокумент11 страницSong Et Al 2007 Thyroid HormonesSyifa Mahmud Syukran AkbarОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Cardiovascular Physical Examination - SyifaДокумент66 страницCardiovascular Physical Examination - SyifaSyifa Mahmud Syukran AkbarОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- AFib GuidlinesДокумент4 страницыAFib GuidlinesSyifa Mahmud Syukran AkbarОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Naskah Publikasi PJB Fix ENGLISH - EditorДокумент8 страницNaskah Publikasi PJB Fix ENGLISH - EditorSyifa Mahmud Syukran AkbarОценок пока нет
- Eutiroid Sick SindromeДокумент8 страницEutiroid Sick SindromeSyifa Mahmud Syukran AkbarОценок пока нет
- The Clinical Importance of Visceral AdiposityДокумент10 страницThe Clinical Importance of Visceral AdiposityKaka Citta PrasiddhaОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Hematologi ModulДокумент67 страницHematologi ModulSyifa Mahmud Syukran Akbar100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Comparison ChadScore & HasBleedДокумент5 страницComparison ChadScore & HasBleedSyifa Mahmud Syukran AkbarОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Living With Atrial FibrilationДокумент20 страницLiving With Atrial FibrilationSyifa Mahmud Syukran AkbarОценок пока нет
- Unlock-04. Neurologi MANTAPДокумент152 страницыUnlock-04. Neurologi MANTAPSyifa Mahmud Syukran AkbarОценок пока нет
- AF and CardiomyopathyДокумент2 страницыAF and CardiomyopathySyifa Mahmud Syukran AkbarОценок пока нет
- Case Study Amanda Loscerbo Atrial FibrilationДокумент6 страницCase Study Amanda Loscerbo Atrial FibrilationSyifa Mahmud Syukran AkbarОценок пока нет
- Bronchiolitis CPGДокумент8 страницBronchiolitis CPGSyifa Mahmud Syukran AkbarОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- BBBДокумент47 страницBBBSyifa Mahmud Syukran AkbarОценок пока нет
- Management & Complications of EVDДокумент4 страницыManagement & Complications of EVDSyifa Mahmud Syukran AkbarОценок пока нет
- Bio209 SarsДокумент35 страницBio209 SarsANDRE ASОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
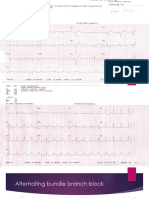
- Alternating Bundle Branch BlockДокумент9 страницAlternating Bundle Branch BlockSyifa Mahmud Syukran AkbarОценок пока нет
- Efek Kristaloid & Koloid Preload On Cardiac Output in SC With SpinalДокумент6 страницEfek Kristaloid & Koloid Preload On Cardiac Output in SC With SpinalSyifa Mahmud Syukran AkbarОценок пока нет
- Local and Regional AnesthesiaДокумент12 страницLocal and Regional AnesthesiaSyifa Mahmud Syukran AkbarОценок пока нет
- Guidelines For The Management of DepressionДокумент3 страницыGuidelines For The Management of DepressionSyifa Mahmud Syukran AkbarОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- KaufmanДокумент2 страницыKaufmanrbtakemotoОценок пока нет
- Pre Op MNGMNTДокумент22 страницыPre Op MNGMNTsandeepv08Оценок пока нет
- Self Myofascial Trigger Point Release Guide PDFДокумент96 страницSelf Myofascial Trigger Point Release Guide PDFCarlos RozoОценок пока нет
- Essential Vocabulary For NursesДокумент6 страницEssential Vocabulary For Nursesbianca_aburelОценок пока нет
- (ACC ENGLISH) ASKEP HiperglikemiaДокумент11 страниц(ACC ENGLISH) ASKEP HiperglikemiaWenОценок пока нет
- Pain and Fever in The PharmacyДокумент11 страницPain and Fever in The PharmacyP D SpencerОценок пока нет
- Acute Pain RT Surgical IncisionДокумент1 страницаAcute Pain RT Surgical Incisiondude06blumОценок пока нет
- Pain ManagementДокумент39 страницPain Managementsteven saputra100% (1)
- Ketamine Presentation - PPT RevisedДокумент31 страницаKetamine Presentation - PPT RevisedJack TanОценок пока нет
- Microcurrent Instructions PDFДокумент11 страницMicrocurrent Instructions PDFFuh Ken Chin100% (1)
- Doctor Ilene EbookДокумент11 страницDoctor Ilene EbookNikhil BhavsarОценок пока нет
- Management of Neck Pain and Associated DisordersДокумент24 страницыManagement of Neck Pain and Associated DisordersManuel OlarteОценок пока нет
- PCEP-PC Module 4 (Pain) NotesДокумент12 страницPCEP-PC Module 4 (Pain) NotesMan MedОценок пока нет
- Infrared and Wax TherapyДокумент20 страницInfrared and Wax Therapyvamshi gundepanguОценок пока нет
- The MELT Method by Sue HitzmannДокумент20 страницThe MELT Method by Sue HitzmannHarperOne (an imprint of HarperCollins)67% (6)
- Physical Therapy Initial Evaluation: PT Seminar 1Документ4 страницыPhysical Therapy Initial Evaluation: PT Seminar 1Katrina Vea CalaroОценок пока нет
- Most Common Used FDAR For Ortho WardДокумент19 страницMost Common Used FDAR For Ortho WardMiguelito Galagar Gultiano75% (4)
- Nursing Care PlanДокумент53 страницыNursing Care PlanAsma AlsaketОценок пока нет
- Pathologic Basis of Lumbar Radicular Pain: BackgroundДокумент8 страницPathologic Basis of Lumbar Radicular Pain: BackgroundVizaОценок пока нет
- Bilateral Enucleation in Dogs: A Review of Owner Perceptions and SatisfactionДокумент11 страницBilateral Enucleation in Dogs: A Review of Owner Perceptions and SatisfactionMark Afandy Fitrah MОценок пока нет
- Tens PDFДокумент62 страницыTens PDFJay Muhammad100% (1)
- Psychological Facts: You Can't Multi-TaskДокумент2 страницыPsychological Facts: You Can't Multi-TaskZegera MgendiОценок пока нет
- Concept Map 6 WДокумент1 страницаConcept Map 6 Wapi-298146834Оценок пока нет
- MalamedДокумент7 страницMalamedProgynanika BarmanОценок пока нет
- Case 1Документ7 страницCase 1Jullienne Ysabelle AngОценок пока нет
- Arthritis Reversed BookДокумент284 страницыArthritis Reversed Bookamitrathee09100% (14)
- Jurnal Nyeri 1Документ10 страницJurnal Nyeri 1Elly SufriadiОценок пока нет
- Complications During Root Canal Irrigation - Literature Review and Case ReportsДокумент8 страницComplications During Root Canal Irrigation - Literature Review and Case ReportsGavi GazОценок пока нет
- Treating Musculo-Skeletal Pain With Traditional Chinese MedicineДокумент2 страницыTreating Musculo-Skeletal Pain With Traditional Chinese MedicineocoxodoОценок пока нет
- Eim4 V 02 WorksheetДокумент1 страницаEim4 V 02 WorksheetSamantha LaneОценок пока нет
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)