Вам также может понравиться
- Palliative Care and Oncology in Colombia The PotenДокумент5 страницPalliative Care and Oncology in Colombia The PotenLina MarcelaОценок пока нет
- Andre, 2016. Embedding Evidence-Based Practice Among Nursing UndergraduatesДокумент6 страницAndre, 2016. Embedding Evidence-Based Practice Among Nursing UndergraduatesLina MarcelaОценок пока нет
- Brooke2015 Student Nurse Perceptions On Evidence-Based Practice and ResearchДокумент6 страницBrooke2015 Student Nurse Perceptions On Evidence-Based Practice and ResearchLina MarcelaОценок пока нет
- Al Qadire, 2019. Undergraduate Student Nurses' Knowledge of Evidence-Based Practice - A Short Online SurveyДокумент5 страницAl Qadire, 2019. Undergraduate Student Nurses' Knowledge of Evidence-Based Practice - A Short Online SurveyLina MarcelaОценок пока нет
- Survivor in The Cancer Context - A Concept AnalysisДокумент13 страницSurvivor in The Cancer Context - A Concept AnalysisLina MarcelaОценок пока нет
- Mishel1984 Perceived Uncertainty and Stress in IllnessДокумент10 страницMishel1984 Perceived Uncertainty and Stress in IllnessLina MarcelaОценок пока нет
- Marzorati2017 Article WhoIsACancerSurvivorASystematiДокумент10 страницMarzorati2017 Article WhoIsACancerSurvivorASystematiLina MarcelaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Yeb2019 Template MhayДокумент9 страницYeb2019 Template MhayloretaОценок пока нет
- 2016 ILA Berlin Air Show June 1 - 4Документ11 страниц2016 ILA Berlin Air Show June 1 - 4sean JacobsОценок пока нет
- Certificat: S Ent of Ivth M T R A Y S Fte O Ogy B NG Ore. H Und R On G N U Organ A Ion Durin The E A C 2 8Документ71 страницаCertificat: S Ent of Ivth M T R A Y S Fte O Ogy B NG Ore. H Und R On G N U Organ A Ion Durin The E A C 2 8Chetana YadawadОценок пока нет
- HTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133Документ3 страницыHTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133hadia duraniОценок пока нет
- Aldehydes and Ketones LectureДокумент21 страницаAldehydes and Ketones LectureEvelyn MushangweОценок пока нет
- Security Operating Procedures and StandardsДокумент5 страницSecurity Operating Procedures and StandardsQuy Tranxuan100% (2)
- Commercial Dispatch Eedition 6-13-19Документ12 страницCommercial Dispatch Eedition 6-13-19The Dispatch100% (1)
- Juzaili Alias SSB Jadual Perubahan PDP Dan Penilaian AlternatifДокумент1 страницаJuzaili Alias SSB Jadual Perubahan PDP Dan Penilaian Alternatifkar afiОценок пока нет
- Preparatory Surface Cleaning of Architectural Sandstone: Standard Practice ForДокумент2 страницыPreparatory Surface Cleaning of Architectural Sandstone: Standard Practice Fors.swamyОценок пока нет
- Product Bulletin Fisher 8580 Rotary Valve en 123032Документ16 страницProduct Bulletin Fisher 8580 Rotary Valve en 123032Rachmat MaulanaОценок пока нет
- 659.69 BM67 2018-02-06 02 Im Beu-UsaДокумент88 страниц659.69 BM67 2018-02-06 02 Im Beu-UsaIrakli JibladzeОценок пока нет
- Look 4 - Unit 4Документ14 страницLook 4 - Unit 4Noura AdhamОценок пока нет
- Making A Spiritual ConfessionДокумент2 страницыMaking A Spiritual ConfessionJoselito FernandezОценок пока нет
- Huawei Videoconferencing MCU VP9600 Series Data SheetДокумент2 страницыHuawei Videoconferencing MCU VP9600 Series Data SheetIsaac PiresОценок пока нет
- Technical ReportДокумент39 страницTechnical ReportTope-Akanni AyomideОценок пока нет
- Dragon Is The Fifth in The 12Документ3 страницыDragon Is The Fifth in The 12Waylon CahiligОценок пока нет
- Affidavit of SeparationДокумент1 страницаAffidavit of SeparationRaysunArellano100% (9)
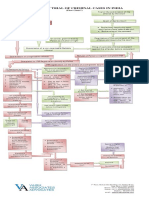
- Process of Trial of Criminal Cases in India (Flow Chart)Документ1 страницаProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Owners Manual Goodman GPC GPHДокумент49 страницOwners Manual Goodman GPC GPHJuan José SanchezОценок пока нет
- QuizДокумент15 страницQuizGracie ChongОценок пока нет
- Csa Case Scenario Stressed GP 2020Документ5 страницCsa Case Scenario Stressed GP 2020pgzhxqscjxciejmpfОценок пока нет
- Investment ChecklistДокумент3 страницыInvestment ChecklistArpan chakrabortyОценок пока нет
- 20 Đề thi thử tốt nghiệp THPT năm 2021 - có đáp ánДокумент131 страница20 Đề thi thử tốt nghiệp THPT năm 2021 - có đáp ánThanh NganОценок пока нет
- Tribebook Wendigo Revised Edition 6244638Документ109 страницTribebook Wendigo Revised Edition 6244638PedroОценок пока нет
- SMEC01 CBRS Guide For NBC Reports - v1.1Документ53 страницыSMEC01 CBRS Guide For NBC Reports - v1.1phal sovannarithОценок пока нет
- Resume Kantesh MundaragiДокумент3 страницыResume Kantesh MundaragiKanteshОценок пока нет
- Case Study 1 - Whirlpool Reverser Logistics - With New Rubric - Winter 2022Документ4 страницыCase Study 1 - Whirlpool Reverser Logistics - With New Rubric - Winter 2022ShravanОценок пока нет
- TLE10 - Q3 - Lesson 5Документ17 страницTLE10 - Q3 - Lesson 5Ella Cagadas PuzonОценок пока нет
- Math9 - Q2 - Mod2 - WK 3 - JointAndCombinedVariations - Version2Документ37 страницMath9 - Q2 - Mod2 - WK 3 - JointAndCombinedVariations - Version2Precious Arni100% (7)
- List - of - Members As On 6 3 18 PDFДокумент8 страницList - of - Members As On 6 3 18 PDFashish jaiswal100% (1)