Вам также может понравиться
- Medical Students' Endeavor To Make Use of Their Mental CapabilitiesДокумент6 страницMedical Students' Endeavor To Make Use of Their Mental CapabilitiesGauri ShahОценок пока нет
- Traditional and Western Medicine: Voices from Jamaican Psychiatric PatientsОт EverandTraditional and Western Medicine: Voices from Jamaican Psychiatric PatientsОценок пока нет
- Nolen-Hoeksema (2004)Документ6 страницNolen-Hoeksema (2004)briancrowder12Оценок пока нет
- Treating Adult Survivors Childhood Emotional Abuse Neglect G0003 PDFДокумент8 страницTreating Adult Survivors Childhood Emotional Abuse Neglect G0003 PDFColten KollenbornОценок пока нет
- How Can Students Diagnostic Competence Benefit.32Документ7 страницHow Can Students Diagnostic Competence Benefit.32Carlos Roberto Pires de Oliveira LimaОценок пока нет
- Dabon, Keyle Ann F. Quiambao, Rosel E. Santos, Jewel Anne DДокумент9 страницDabon, Keyle Ann F. Quiambao, Rosel E. Santos, Jewel Anne DJewel Anne SantosОценок пока нет
- An Interdisciplinary Community Diagnosis Experience in An Undergraduate Medical Curriculum: Development at Ghent UniversityДокумент9 страницAn Interdisciplinary Community Diagnosis Experience in An Undergraduate Medical Curriculum: Development at Ghent UniversityEgi NabilaОценок пока нет
- Potential Predictors of Psychological DistressДокумент11 страницPotential Predictors of Psychological DistressJose Angel LopezОценок пока нет
- The Stigma ScaleДокумент8 страницThe Stigma ScaleIka JuitaОценок пока нет
- E-Hidden in Plain Sight The Formal Informal and Hidden Curricula of A Psychiatry ClerkshipДокумент8 страницE-Hidden in Plain Sight The Formal Informal and Hidden Curricula of A Psychiatry Clerkshipusman sajidОценок пока нет
- Engel 1980 The Clinical Application of of The Biopsychosocial Model PDFДокумент10 страницEngel 1980 The Clinical Application of of The Biopsychosocial Model PDFDiego Almanza HolguinОценок пока нет
- Wakefiled (1992)Документ16 страницWakefiled (1992)Danusia JОценок пока нет
- Navarro, General Trias City, Cavite: Senior High School DepartmentДокумент5 страницNavarro, General Trias City, Cavite: Senior High School DepartmentVan TracilynОценок пока нет
- Understanding Families' Experiences Non-SyndromicДокумент8 страницUnderstanding Families' Experiences Non-Syndromiccristobal.mezaОценок пока нет
- Demographic, Personality, and Social Cognition Correlates of Coronavirus Guideline Adherence in A U.S. SampleДокумент11 страницDemographic, Personality, and Social Cognition Correlates of Coronavirus Guideline Adherence in A U.S. Samplesayyid cbrОценок пока нет
- TANAKA Et Al-2005-Psychiatry and Clinical NeurosciencesДокумент6 страницTANAKA Et Al-2005-Psychiatry and Clinical NeurosciencesBakrОценок пока нет
- Evidence For A Mental Health Crisis in Graduate EducationДокумент3 страницыEvidence For A Mental Health Crisis in Graduate EducationJeferson BarbosaОценок пока нет
- 10 1038@nbt 4089 PDFДокумент3 страницы10 1038@nbt 4089 PDFAnonymous DSATBjОценок пока нет
- (1930) BOHANNAN - Mental Hygiene From The Standpoint of College Administration 1930Документ16 страниц(1930) BOHANNAN - Mental Hygiene From The Standpoint of College Administration 1930Thiago Marques LeãoОценок пока нет
- 27716335Документ3 страницы27716335Mark BenОценок пока нет
- Med Research Imposter Syndrome Proposal CsuДокумент38 страницMed Research Imposter Syndrome Proposal CsuRuth Anne Sharmaine SantosОценок пока нет
- Psychology 2Документ10 страницPsychology 2PandaОценок пока нет
- Stress, Anxiety and Depression in Students of A Private Medical School in Karachi, PakistanДокумент6 страницStress, Anxiety and Depression in Students of A Private Medical School in Karachi, PakistanRika RatnasariОценок пока нет
- Systematic Review of Depression, Anxiety, and Other Indicators of Psychological Distress Among U.S. and Canadian Medical StudentsДокумент20 страницSystematic Review of Depression, Anxiety, and Other Indicators of Psychological Distress Among U.S. and Canadian Medical StudentsSteven FongОценок пока нет
- Argument SupportationДокумент6 страницArgument SupportationJULIA KooОценок пока нет
- Theorists Phil BarkerДокумент12 страницTheorists Phil BarkerAlleah Mendoza100% (1)
- Social Support and Mental Health Among College StudentsДокумент9 страницSocial Support and Mental Health Among College StudentsIra LampayanОценок пока нет
- Explore The Knowledge and Impact On Dysmenorrhea Among Nursing Students of Selected CollegeДокумент5 страницExplore The Knowledge and Impact On Dysmenorrhea Among Nursing Students of Selected CollegeEditor IJTSRDОценок пока нет
- ResearchДокумент134 страницыResearchMie LОценок пока нет
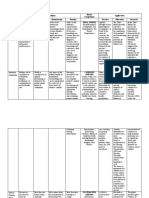
- Methodology of PCДокумент0 страницMethodology of PCShibu MundayatОценок пока нет
- Re-Defining Moral Distress: A Systematic Review and Critical Re-Appraisal of The Argument-Based Bioethics LiteratureДокумент16 страницRe-Defining Moral Distress: A Systematic Review and Critical Re-Appraisal of The Argument-Based Bioethics Literatureadhafauzihendrawan2004Оценок пока нет
- Trauma-Informed SchoolsДокумент17 страницTrauma-Informed SchoolsCamille RichouxОценок пока нет
- Sentinel Emotional Events: The Nature, Triggers, and Effects of Shame Experiences in Medical ResidentsДокумент9 страницSentinel Emotional Events: The Nature, Triggers, and Effects of Shame Experiences in Medical ResidentsYoliset RomeroОценок пока нет
- Georgina ParkerДокумент10 страницGeorgina Parkermsoto20052576Оценок пока нет
- Trauma Informed Aplications of ABAДокумент22 страницыTrauma Informed Aplications of ABACarregan AlvarezОценок пока нет
- NURES Group4 (CU2)Документ8 страницNURES Group4 (CU2)AriaОценок пока нет
- A Qualitative Study of Mental Health Experiences and College StudДокумент109 страницA Qualitative Study of Mental Health Experiences and College Studcatherine oroОценок пока нет
- Reflection In/and Writing: Pedagogy and Practice in Medical EducationДокумент7 страницReflection In/and Writing: Pedagogy and Practice in Medical Educationulices quintanaОценок пока нет
- Effectiveness of Jacobson'S Progressive Muscle Relaxation (JPMR) Technique On Social Anxiety Among High School Adolescents in A Selected School of Udupi District, Karnataka StateДокумент5 страницEffectiveness of Jacobson'S Progressive Muscle Relaxation (JPMR) Technique On Social Anxiety Among High School Adolescents in A Selected School of Udupi District, Karnataka StateSidharth PraveenОценок пока нет
- An Assessment of Suicide-Related Knowledge and Skills Among Health ProfessionalsДокумент10 страницAn Assessment of Suicide-Related Knowledge and Skills Among Health ProfessionalsIshban Wang'ombeОценок пока нет
- Integenerational Transmission of DepressionДокумент26 страницIntegenerational Transmission of DepressionHector LegrekОценок пока нет
- Patient-Centred Attitudes Among Medical Students in Mali, West Africa: A Cross-Sectional StudyДокумент10 страницPatient-Centred Attitudes Among Medical Students in Mali, West Africa: A Cross-Sectional Studyhamayal xОценок пока нет
- Selected College Students Perceptions Knowledge and Awareness oДокумент88 страницSelected College Students Perceptions Knowledge and Awareness oDiksha chaudharyОценок пока нет
- The Construction of Fear Americans PrefeДокумент19 страницThe Construction of Fear Americans Prefeega meilindraОценок пока нет
- Effects of A Risk and Resilience Course On Stress, Coping Skills, and Cognitive Strategies in College StudentsДокумент7 страницEffects of A Risk and Resilience Course On Stress, Coping Skills, and Cognitive Strategies in College StudentscrazyappleОценок пока нет
- E144 Vol. 52 No. 6 December 2016 Selected AbstractsДокумент2 страницыE144 Vol. 52 No. 6 December 2016 Selected AbstractsJos CanalesОценок пока нет
- OutДокумент127 страницOutMai MimiОценок пока нет
- (Bradford Books) Prinz, Wolfgang - Sebanz, Natalie - Disorders of Volition-The MIT Press (2006)Документ502 страницы(Bradford Books) Prinz, Wolfgang - Sebanz, Natalie - Disorders of Volition-The MIT Press (2006)Víctor FuentesОценок пока нет
- LGBT 2020 0494Документ9 страницLGBT 2020 0494Belén DobrichОценок пока нет
- 2016-The - Clinical - Teacher (Clinical Teaching Lesson Plan)Документ2 страницы2016-The - Clinical - Teacher (Clinical Teaching Lesson Plan)Justin VergaraОценок пока нет
- ABowman Dissertatio FinalДокумент133 страницыABowman Dissertatio FinalManu JimenezОценок пока нет
- The Associations Between University Adjustment AduДокумент13 страницThe Associations Between University Adjustment AduAna Maria NОценок пока нет
- Anxiety in Children With Autism Spectrum Disorders - An ExaminatioДокумент138 страницAnxiety in Children With Autism Spectrum Disorders - An ExaminatioFakher KhaliliОценок пока нет
- The Role of Psychological Flexibility in Graduate Student StressДокумент144 страницыThe Role of Psychological Flexibility in Graduate Student StressYuva RaniОценок пока нет
- Current Concepts in Feminizing Gender Surgery.46Документ11 страницCurrent Concepts in Feminizing Gender Surgery.46Razaria DailyneОценок пока нет
- TeachingДокумент6 страницTeachingmelanieОценок пока нет
- 3-Characteristics of The Informal CurriculumДокумент10 страниц3-Characteristics of The Informal CurriculumKОценок пока нет
- Bmjopen-2020-046654 Kohort (M7)Документ8 страницBmjopen-2020-046654 Kohort (M7)rsandal1997Оценок пока нет
- Dorothy Johnson Theory PDFДокумент7 страницDorothy Johnson Theory PDFJenny SorianoОценок пока нет
- OB Journal AppraisalДокумент2 страницыOB Journal AppraisalAlloiBialbaОценок пока нет
- Reflection 6Документ2 страницыReflection 6AlloiBialbaОценок пока нет
- Health Care For PublishДокумент99 страницHealth Care For PublishAlloiBialbaОценок пока нет
- (Template) PediaДокумент7 страниц(Template) PediaAlloiBialbaОценок пока нет
- Alloi: Li, X., Et Al. (2020)Документ2 страницыAlloi: Li, X., Et Al. (2020)AlloiBialbaОценок пока нет
- Bialba TB PharmaДокумент2 страницыBialba TB PharmaAlloiBialbaОценок пока нет
- (Surg2) 5.2 Urology Part 1 - Dr. YusiДокумент18 страниц(Surg2) 5.2 Urology Part 1 - Dr. YusiAlloiBialbaОценок пока нет
- Case LegMedДокумент1 страницаCase LegMedAlloiBialbaОценок пока нет
- CAP Nelsons DR - Atienza 2020-2021Документ15 страницCAP Nelsons DR - Atienza 2020-2021AlloiBialbaОценок пока нет
- (Surg2) 5.1a Introduction To Anesthesia Part 1Документ21 страница(Surg2) 5.1a Introduction To Anesthesia Part 1AlloiBialbaОценок пока нет
- (Surg2) 5.4 Urology Part 3Документ23 страницы(Surg2) 5.4 Urology Part 3AlloiBialbaОценок пока нет
- Wooten Review ArticleДокумент9 страницWooten Review ArticleAlloiBialbaОценок пока нет
- Pharmacotherapeutic (Medpharma30) AY 2020-2021 Treatment Drug SelectionДокумент2 страницыPharmacotherapeutic (Medpharma30) AY 2020-2021 Treatment Drug SelectionAlloiBialbaОценок пока нет
- (Surg2) 5.1c Anesthesia Video TranscriptionДокумент5 страниц(Surg2) 5.1c Anesthesia Video TranscriptionAlloiBialbaОценок пока нет
- Over-the-Counter Medications in PregnancyДокумент8 страницOver-the-Counter Medications in PregnancyAlloiBialbaОценок пока нет
- (Surg2) 5.1b Introduction To Anesthesia-Part 2Документ16 страниц(Surg2) 5.1b Introduction To Anesthesia-Part 2AlloiBialbaОценок пока нет
- (Surg2) 5.3 Urology Part 2 - Dr. YusiДокумент19 страниц(Surg2) 5.3 Urology Part 2 - Dr. YusiAlloiBialbaОценок пока нет
- Paediatric Pharmacokinetics: Key Considerations: Hannah Katharine Batchelor & John Francis MarriottДокумент10 страницPaediatric Pharmacokinetics: Key Considerations: Hannah Katharine Batchelor & John Francis MarriottAlloiBialbaОценок пока нет
- Pharmacotherapy During Pregnancy, Childbirth and LactationДокумент6 страницPharmacotherapy During Pregnancy, Childbirth and Lactationfiras frsОценок пока нет
- Surger YII Clinic AL Case: Group 4B Bernabe, Bernardo, Bialba, BigorniaДокумент39 страницSurger YII Clinic AL Case: Group 4B Bernabe, Bernardo, Bialba, BigorniaAlloiBialbaОценок пока нет
- Paediatric Pharmacokinetics: Key Considerations: Hannah Katharine Batchelor & John Francis MarriottДокумент10 страницPaediatric Pharmacokinetics: Key Considerations: Hannah Katharine Batchelor & John Francis MarriottAlloiBialbaОценок пока нет
- Good Prescribing GuideДокумент142 страницыGood Prescribing GuideTheresa ValleriОценок пока нет
- Pharmacology: Outline PharmacodynamicsДокумент11 страницPharmacology: Outline PharmacodynamicsAlloiBialbaОценок пока нет
- (Surg2) 5.1d Anesthesia PointersДокумент12 страниц(Surg2) 5.1d Anesthesia PointersAlloiBialbaОценок пока нет
- Don't Use AbbreviationДокумент3 страницыDon't Use AbbreviationSara tarekОценок пока нет
- Rational Prescribing: The Principles of Drug Selection: Author: Simon RJ MaxwellДокумент6 страницRational Prescribing: The Principles of Drug Selection: Author: Simon RJ MaxwellAlloiBialbaОценок пока нет
- Tratamiento - Integral.de - Las.quemaduras EspañolДокумент21 страницаTratamiento - Integral.de - Las.quemaduras EspañolPablo HenríquezОценок пока нет
- Neuropreceptorial ChecklistДокумент33 страницыNeuropreceptorial ChecklistAlloiBialba0% (1)
- Neuropreceptorial ChecklistДокумент33 страницыNeuropreceptorial ChecklistAlloiBialba0% (1)
- Standard Operating ProceduresДокумент89 страницStandard Operating ProceduresAsfa JaVed100% (11)
- Cultivating Empathy For The Mentally Ill Using Simulated Auditory HallucinationsДокумент4 страницыCultivating Empathy For The Mentally Ill Using Simulated Auditory HallucinationsGloria Carbajal ZegarraОценок пока нет
- MSPE Noteworthy Characteristics Worksheet: Complete This Worksheet and Bring It To Your Mandatory Career Advising SessionДокумент2 страницыMSPE Noteworthy Characteristics Worksheet: Complete This Worksheet and Bring It To Your Mandatory Career Advising SessionHải Dương NguyễnОценок пока нет
- Clinical Sports MedicineДокумент729 страницClinical Sports MedicineRugiada222100% (2)
- Henry Ford Macomb Hospital ProgramДокумент26 страницHenry Ford Macomb Hospital ProgramRamanpreet Kaur MaanОценок пока нет
- Islamic Perspective Written ReportДокумент8 страницIslamic Perspective Written ReportAbegail JutbaОценок пока нет
- XJXNDДокумент56 страницXJXNDGautam NatrajОценок пока нет
- John FlynnsДокумент10 страницJohn Flynnssamwong87Оценок пока нет
- Medical Ethics: Indian Journal ofДокумент76 страницMedical Ethics: Indian Journal ofkaarkkiОценок пока нет
- Insan Anatomisi Atlasi Mcminn 1515167549Документ18 страницInsan Anatomisi Atlasi Mcminn 1515167549Müslüm ŞahinОценок пока нет
- Allied Health Sciences: The Tamilnadu Dr. M.G.R. Medical UniversityДокумент4 страницыAllied Health Sciences: The Tamilnadu Dr. M.G.R. Medical Universitysasenthil241464Оценок пока нет
- Cover Letter For Medical OfficerДокумент8 страницCover Letter For Medical Officerbcqvdfyg100% (2)
- Rockefeller Foundation RapportДокумент477 страницRockefeller Foundation RapportundermattanОценок пока нет
- Choosing A Medical School & MD-PHD Program: A Black Student's GuideДокумент16 страницChoosing A Medical School & MD-PHD Program: A Black Student's GuideAyomide OjebuobohОценок пока нет
- Who MC Topic-6Документ14 страницWho MC Topic-6Kartika Radianti WardhaniОценок пока нет
- Research 1st Year Med StudentsДокумент26 страницResearch 1st Year Med StudentsMutasimОценок пока нет
- Becoming A DoctorДокумент5 страницBecoming A DoctorInzi AsadОценок пока нет
- Journal of Health Global 2018Документ344 страницыJournal of Health Global 2018Rizki Agung PrasetyoОценок пока нет
- A New Leadership Curriculum: The Multiplication of IntelligenceДокумент4 страницыA New Leadership Curriculum: The Multiplication of IntelligenceGisele PhaloОценок пока нет
- SWU Orientation Surgery 2Документ17 страницSWU Orientation Surgery 2Jabagat, Benedict Christian P.Оценок пока нет
- Hong Kong's First Professor of Pathology and The Laboratory of The Royal College of Physicians of EdinburghДокумент6 страницHong Kong's First Professor of Pathology and The Laboratory of The Royal College of Physicians of EdinburghJhonalValdimirQuispeMamaniОценок пока нет
- Communication Skills Education For Doctors: An UpdateДокумент50 страницCommunication Skills Education For Doctors: An UpdateDaniel PendickОценок пока нет
- 2024-2025 Fulltime Application FormДокумент9 страниц2024-2025 Fulltime Application Formmbewerahab6Оценок пока нет
- KHYBER PAKHTUNKHWA PUBLIC SERVICE COMMISSION AdvertisementДокумент16 страницKHYBER PAKHTUNKHWA PUBLIC SERVICE COMMISSION Advertisementzahoor aliОценок пока нет
- Ebook Goldman Cecil Medicine PDF Full Chapter PDFДокумент67 страницEbook Goldman Cecil Medicine PDF Full Chapter PDFjames.farnan170100% (25)
- Wilson Newsletter September 2020Документ2 страницыWilson Newsletter September 2020Valerie PadillaОценок пока нет
- Problem-Based Learning in Clinical Education The Next Generation by Cindy E. Hmelo-SilverДокумент261 страницаProblem-Based Learning in Clinical Education The Next Generation by Cindy E. Hmelo-Silverjuanc1112Оценок пока нет
- Teresa M Rust Curriculum VitaeДокумент5 страницTeresa M Rust Curriculum Vitaeapi-309387276Оценок пока нет
- Wissenswertes Für Die USA-FamulaturДокумент2 страницыWissenswertes Für Die USA-FamulaturCoskun SuermeliОценок пока нет
- Child and Adolescent Psychiatry - Blackwell's Neurology and Psychiatry Access SeriesДокумент416 страницChild and Adolescent Psychiatry - Blackwell's Neurology and Psychiatry Access SeriesErickson Arthur Siahaan0% (1)
- From Paycheck to Purpose: The Clear Path to Doing Work You LoveОт EverandFrom Paycheck to Purpose: The Clear Path to Doing Work You LoveРейтинг: 4.5 из 5 звезд4.5/5 (39)
- The 7 Habits of Highly Effective People: The Infographics EditionОт EverandThe 7 Habits of Highly Effective People: The Infographics EditionРейтинг: 4 из 5 звезд4/5 (2475)
- Summary: 12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure Entrepreneur by Ryan Daniel Moran: Key Takeaways, Summary & AnalysisОт EverandSummary: 12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure Entrepreneur by Ryan Daniel Moran: Key Takeaways, Summary & AnalysisРейтинг: 5 из 5 звезд5/5 (2)
- The 30 Day MBA: Your Fast Track Guide to Business SuccessОт EverandThe 30 Day MBA: Your Fast Track Guide to Business SuccessРейтинг: 4.5 из 5 звезд4.5/5 (19)
- Designing Your Life by Bill Burnett, Dave Evans - Book Summary: How to Build a Well-Lived, Joyful LifeОт EverandDesigning Your Life by Bill Burnett, Dave Evans - Book Summary: How to Build a Well-Lived, Joyful LifeРейтинг: 4.5 из 5 звезд4.5/5 (62)
- The Proximity Principle: The Proven Strategy That Will Lead to the Career You LoveОт EverandThe Proximity Principle: The Proven Strategy That Will Lead to the Career You LoveРейтинг: 4.5 из 5 звезд4.5/5 (93)
- Start.: Punch Fear in the Face, Escape Average, and Do Work That MattersОт EverandStart.: Punch Fear in the Face, Escape Average, and Do Work That MattersРейтинг: 4.5 из 5 звезд4.5/5 (56)
- Steal the Show: From Speeches to Job Interviews to Deal-Closing Pitches, How to Guarantee a Standing Ovation for All the Performances in Your LifeОт EverandSteal the Show: From Speeches to Job Interviews to Deal-Closing Pitches, How to Guarantee a Standing Ovation for All the Performances in Your LifeРейтинг: 4.5 из 5 звезд4.5/5 (39)
- Work Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkОт EverandWork Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkРейтинг: 4.5 из 5 звезд4.5/5 (12)
- The First 90 Days: Proven Strategies for Getting Up to Speed Faster and SmarterОт EverandThe First 90 Days: Proven Strategies for Getting Up to Speed Faster and SmarterРейтинг: 4.5 из 5 звезд4.5/5 (122)
- The Business of Beauty: Your Guide To Happiness And Success In The Salon IndustryОт EverandThe Business of Beauty: Your Guide To Happiness And Success In The Salon IndustryРейтинг: 3.5 из 5 звезд3.5/5 (2)
- The 2-Hour Job Search: Using Technology to Get the Right Job FasterОт EverandThe 2-Hour Job Search: Using Technology to Get the Right Job FasterРейтинг: 4 из 5 звезд4/5 (23)
- The 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsОт EverandThe 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsРейтинг: 4.5 из 5 звезд4.5/5 (90)
- 12 Habits Of Valuable Employees: Your Roadmap to an Amazing CareerОт Everand12 Habits Of Valuable Employees: Your Roadmap to an Amazing CareerОценок пока нет
- The Ultimate Sales Letter, 4th Edition: Attract New Customers, Boost Your SalesОт EverandThe Ultimate Sales Letter, 4th Edition: Attract New Customers, Boost Your SalesРейтинг: 4.5 из 5 звезд4.5/5 (98)
- The Power of Body Language: An Ex-FBI Agent's System for Speed-Reading PeopleОт EverandThe Power of Body Language: An Ex-FBI Agent's System for Speed-Reading PeopleРейтинг: 5 из 5 звезд5/5 (9)
- The Everything Guide To Being A Paralegal: Winning Secrets to a Successful Career!От EverandThe Everything Guide To Being A Paralegal: Winning Secrets to a Successful Career!Рейтинг: 5 из 5 звезд5/5 (1)
- What Every BODY is Saying: An Ex-FBI Agent’s Guide to Speed-Reading PeopleОт EverandWhat Every BODY is Saying: An Ex-FBI Agent’s Guide to Speed-Reading PeopleРейтинг: 4.5 из 5 звезд4.5/5 (354)
- Company Of One: Why Staying Small Is the Next Big Thing for BusinessОт EverandCompany Of One: Why Staying Small Is the Next Big Thing for BusinessРейтинг: 3.5 из 5 звезд3.5/5 (14)
- Happy at Work: How to Create a Happy, Engaging Workplace for Today's (and Tomorrow's!) WorkforceОт EverandHappy at Work: How to Create a Happy, Engaging Workplace for Today's (and Tomorrow's!) WorkforceОценок пока нет
- Real Artists Don't Starve: Timeless Strategies for Thriving in the New Creative AgeОт EverandReal Artists Don't Starve: Timeless Strategies for Thriving in the New Creative AgeРейтинг: 4.5 из 5 звезд4.5/5 (197)
- Ultralearning: Master Hard Skills, Outsmart the Competition, and Accelerate Your CareerОт EverandUltralearning: Master Hard Skills, Outsmart the Competition, and Accelerate Your CareerРейтинг: 4.5 из 5 звезд4.5/5 (360)
- Got Your Attention?: How to Create Intrigue and Connect with AnyoneОт EverandGot Your Attention?: How to Create Intrigue and Connect with AnyoneРейтинг: 4.5 из 5 звезд4.5/5 (4)