Вам также может понравиться
- Manual G Ingles - V6Документ68 страницManual G Ingles - V6Phùng Thế Kiên50% (2)
- PS-8955 Zinc Alloy ElectrodepositedДокумент8 страницPS-8955 Zinc Alloy ElectrodepositedArturo Palacios100% (1)
- 10 1016@j JHT 2017 02 001 PDFДокумент10 страниц10 1016@j JHT 2017 02 001 PDFGusti Ayu KrisnayantiОценок пока нет
- Cairns 2006Документ12 страницCairns 2006David LorencОценок пока нет
- Pulsed Radiofrequency ofДокумент8 страницPulsed Radiofrequency ofDiego Pinto PatroniОценок пока нет
- Albert Et Al. The Efficacy of Systematic Active Conservative Treatment For Patients With Severe Sciatica - AbstractДокумент2 страницыAlbert Et Al. The Efficacy of Systematic Active Conservative Treatment For Patients With Severe Sciatica - AbstractPremanandi Devi DasiОценок пока нет
- Fritz 2003Документ10 страницFritz 2003Sandro PerilloОценок пока нет
- 2002 Jull - A Randomized Controlled Trial of ExercisДокумент9 страниц2002 Jull - A Randomized Controlled Trial of ExercisFernando ImazОценок пока нет
- The Treatment of Acute Low Back Pain - Bed Rest, Exercises, or Ordinary Activity?Документ5 страницThe Treatment of Acute Low Back Pain - Bed Rest, Exercises, or Ordinary Activity?Arya Maulana NugrohoОценок пока нет
- A Comparison of Osteopathic Spinal Manipulation With Standard Nejm199911043411903Документ6 страницA Comparison of Osteopathic Spinal Manipulation With Standard Nejm199911043411903Paola GuerraОценок пока нет
- Brennan Et Al Spine 2006 RCT LBPДокумент9 страницBrennan Et Al Spine 2006 RCT LBPEric ZhangОценок пока нет
- Malone Final SignedДокумент29 страницMalone Final Signedapi-622666324Оценок пока нет
- Journal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDДокумент9 страницJournal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDWinda FRОценок пока нет
- Journal Pone 0193358Документ20 страницJournal Pone 0193358Emad Eldin Mohamed AbdelatiefОценок пока нет
- Atlas SPINE 2001Документ9 страницAtlas SPINE 2001yudhafpОценок пока нет
- Acupuncture For Acute Non-Speci Fic Low Back Pain: A Protocol For A Randomised, Controlled Multicentre Intervention Study in General Practicedthe Acuback StudyДокумент9 страницAcupuncture For Acute Non-Speci Fic Low Back Pain: A Protocol For A Randomised, Controlled Multicentre Intervention Study in General Practicedthe Acuback StudyNashrullohNAkbarОценок пока нет
- The Effectiveness and Safety of Manual Therapy On Pain and Disability in Older Persons With Chronic Low Back Pain: A Systematic ReviewДокумент8 страницThe Effectiveness and Safety of Manual Therapy On Pain and Disability in Older Persons With Chronic Low Back Pain: A Systematic ReviewCleyber SantosОценок пока нет
- PT Hip-OA 2014Документ11 страницPT Hip-OA 2014GeorgeKielingОценок пока нет
- Maik SLR and Slump Stretching With LBP Neural TensionДокумент9 страницMaik SLR and Slump Stretching With LBP Neural TensionFallahPhysioОценок пока нет
- Flynn2002 PDFДокумент9 страницFlynn2002 PDFMuhammad JuniarsyahОценок пока нет
- Effectiveness of Core Stabilization Exercises and Routine Exercise Therapy in Management of Pain in Chronic Non-Specific Low Back Pain A Randomized Controlled Clinical Trial PDFДокумент5 страницEffectiveness of Core Stabilization Exercises and Routine Exercise Therapy in Management of Pain in Chronic Non-Specific Low Back Pain A Randomized Controlled Clinical Trial PDFFelipe solis jimenez100% (1)
- Acupuncture PDFДокумент9 страницAcupuncture PDFGrafika DiahОценок пока нет
- 12 Suppl - 4 S119Документ9 страниц12 Suppl - 4 S119Dr AliОценок пока нет
- Michel IzquierdoДокумент3 страницыMichel IzquierdoEsmeralda09Оценок пока нет
- Comments Fritz Jama EBM2016Документ1 страницаComments Fritz Jama EBM2016Ju ChangОценок пока нет
- A Randomized Controlled Trial of Exercise and Manipulative Therapy For Cervicogenic HeadacheДокумент9 страницA Randomized Controlled Trial of Exercise and Manipulative Therapy For Cervicogenic Headachepaulina_810Оценок пока нет
- Jurnal LBPДокумент10 страницJurnal LBPeka mei dianitaОценок пока нет
- Childs 2004 - Proposal of A Classi Cation System For Patients With Neck PainДокумент15 страницChilds 2004 - Proposal of A Classi Cation System For Patients With Neck PainRogéria RibeiroОценок пока нет
- E000391 FullДокумент10 страницE000391 FullcogajoОценок пока нет
- Subgrouping Patients With Low Back PainДокумент13 страницSubgrouping Patients With Low Back PainVladislav KotovОценок пока нет
- Li 2018Документ7 страницLi 2018Thu TranОценок пока нет
- CV DewiДокумент9 страницCV DewiDewi YulyantiОценок пока нет
- 1 s2.0 S0965229901904819 MainДокумент8 страниц1 s2.0 S0965229901904819 MainSaleha TariqОценок пока нет
- Lower Back PainДокумент18 страницLower Back PainmeganОценок пока нет
- Pone 0203029jsjsjДокумент20 страницPone 0203029jsjsjElizabethBarriaОценок пока нет
- Bronfort2001 2Документ10 страницBronfort2001 2Shaun TylerОценок пока нет
- 7 Effect of Specific Exercise Strategy On Need For Surgery in Patients With Subacromial Impingement Syndrome-Randomised Controlled StudyДокумент3 страницы7 Effect of Specific Exercise Strategy On Need For Surgery in Patients With Subacromial Impingement Syndrome-Randomised Controlled StudyJefferson James Dos SantosОценок пока нет
- A Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategie - 20170730120051Документ8 страницA Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategie - 20170730120051sebafigueroa94Оценок пока нет
- A Randomized Controlled Trial of Ultrasound Guided.39-2Документ5 страницA Randomized Controlled Trial of Ultrasound Guided.39-2Ervin SeborgaОценок пока нет
- Clinical GuidelinesДокумент34 страницыClinical GuidelinesAlberto PachecoОценок пока нет
- Effectiveness of An Extension-OrientedДокумент11 страницEffectiveness of An Extension-OrientedAna Carolina SouzaОценок пока нет
- Negrini 2Документ5 страницNegrini 2iguija6769Оценок пока нет
- Clinical GuidelinesДокумент34 страницыClinical GuidelinesSandro PerilloОценок пока нет
- Effectiveness of Global Postural Re-Education For Treatment of Spinal Disorders A Meta-AnalysisДокумент10 страницEffectiveness of Global Postural Re-Education For Treatment of Spinal Disorders A Meta-AnalysisraquelbibiОценок пока нет
- Jurnal Neuropaty dm2Документ2 страницыJurnal Neuropaty dm2ferryОценок пока нет
- Guided Imagery Relaxation Therapy in Malaysian Patients With Knee Osteoarthritis: A Randomized Controlled TrialДокумент12 страницGuided Imagery Relaxation Therapy in Malaysian Patients With Knee Osteoarthritis: A Randomized Controlled TrialLili YaacobОценок пока нет
- HYDROCHEPALUSДокумент11 страницHYDROCHEPALUSi pentungОценок пока нет
- ShareefДокумент12 страницShareefParaschiva PîțuОценок пока нет
- Instructor: Evidence Based Practice in Physical TherapyДокумент20 страницInstructor: Evidence Based Practice in Physical TherapySameeha AbbassОценок пока нет
- Effect of Mulligan Concept Lumbar SNAG On Chronic Nonspecific Low Back PainДокумент10 страницEffect of Mulligan Concept Lumbar SNAG On Chronic Nonspecific Low Back PainFebryanti Fisio2019Оценок пока нет
- PTJ 1275Документ12 страницPTJ 1275Taynah LopesОценок пока нет
- 4.1.7 Fritz Et Al. Subgroup Traction. 07Документ8 страниц4.1.7 Fritz Et Al. Subgroup Traction. 07Rikita PatelОценок пока нет
- Evidence To Practice Review Best Practices in Patellar Tendinopathy ManagementДокумент8 страницEvidence To Practice Review Best Practices in Patellar Tendinopathy ManagementLeandroОценок пока нет
- Artigo Completo - Subgrupos - CervicalДокумент12 страницArtigo Completo - Subgrupos - CervicalrenatosnacerОценок пока нет
- Clinical Roundup Rheumatoid ArthritisДокумент7 страницClinical Roundup Rheumatoid ArthritisSrikesav SivakumarОценок пока нет
- Paul B. Bishop, DC, MD, PHD, Jeffrey A. Quon, DC, PHD, FCCSC, Charles G. Fisher, MD, MHSC, FRCSC, Marcel F.S. Dvorak, MD, FRCSCДокумент10 страницPaul B. Bishop, DC, MD, PHD, Jeffrey A. Quon, DC, PHD, FCCSC, Charles G. Fisher, MD, MHSC, FRCSC, Marcel F.S. Dvorak, MD, FRCSCorlando moraОценок пока нет
- Hall (2022) - Guía Práctica Clínica RVДокумент60 страницHall (2022) - Guía Práctica Clínica RVElizabeth Fernanda Fuentes100% (1)
- Ger - Errington-Evans, Nick. (2015)Документ5 страницGer - Errington-Evans, Nick. (2015)Rafael ConcursoОценок пока нет
- FritzДокумент12 страницFritzvalentinaro73Оценок пока нет
- Is Cupping Therapy Effective in Patients With Neck Pain? A Systematic Review and Meta-AnalysisДокумент13 страницIs Cupping Therapy Effective in Patients With Neck Pain? A Systematic Review and Meta-AnalysisBruno OliveiraОценок пока нет
- Physical Function in Hospice Patients and Physiotherapy Interventions: A Profile of Hospice PhysiotherapyДокумент8 страницPhysical Function in Hospice Patients and Physiotherapy Interventions: A Profile of Hospice PhysiotherapyAnggita Setya LudtianingmaОценок пока нет
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationОт EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehОценок пока нет
- McKenzie Mechanical Syndromes Coincide With Biopsychosocial InfluencesДокумент14 страницMcKenzie Mechanical Syndromes Coincide With Biopsychosocial InfluencesTomáš KrajíčekОценок пока нет
- PE067 Handout Shoulder Special Tests and The Rotator Cuff With DR Chris LittlewoodДокумент5 страницPE067 Handout Shoulder Special Tests and The Rotator Cuff With DR Chris LittlewoodTomáš KrajíčekОценок пока нет
- PE066 Treatment of Calf Pain in Runners HandoutДокумент3 страницыPE066 Treatment of Calf Pain in Runners HandoutTomáš KrajíčekОценок пока нет
- Tendinopathy Rehabilitation - PhysiopediaДокумент11 страницTendinopathy Rehabilitation - PhysiopediaTomáš KrajíčekОценок пока нет
- PE064 Calf Pain in Runners HandoutДокумент3 страницыPE064 Calf Pain in Runners HandoutTomáš KrajíčekОценок пока нет
- PE 065 InfographicДокумент1 страницаPE 065 InfographicTomáš KrajíčekОценок пока нет
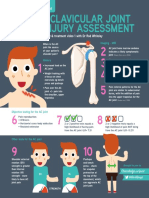
- AC Joint InfographicДокумент1 страницаAC Joint InfographicTomáš KrajíčekОценок пока нет
- Confidence Intervals: Linking Evidence To PracticeДокумент2 страницыConfidence Intervals: Linking Evidence To PracticeTomáš KrajíčekОценок пока нет
- Interpreting Outcomes 3 - Clinical Meaningfulness: Linking Evidence To PracticeДокумент2 страницыInterpreting Outcomes 3 - Clinical Meaningfulness: Linking Evidence To PracticeTomáš KrajíčekОценок пока нет
- Construct Validity of Lumbar Extension Measures in Mckenzie'S Derangement SyndromeДокумент7 страницConstruct Validity of Lumbar Extension Measures in Mckenzie'S Derangement SyndromeTomáš KrajíčekОценок пока нет
- Bias: Linking Evidence With PracticeДокумент2 страницыBias: Linking Evidence With PracticeTomáš KrajíčekОценок пока нет
- 1 PE 067 InfographicДокумент1 страница1 PE 067 InfographicTomáš KrajíčekОценок пока нет
- Generalizability: Linking Evidence To PracticeДокумент2 страницыGeneralizability: Linking Evidence To PracticeTomáš KrajíčekОценок пока нет
- 07 Fundamentals of MeasurementДокумент2 страницы07 Fundamentals of MeasurementTomáš KrajíčekОценок пока нет
- 08 Reliability and ValidityДокумент2 страницы08 Reliability and ValidityTomáš KrajíčekОценок пока нет
- Randomization: Linking Evidence To PracticeДокумент2 страницыRandomization: Linking Evidence To PracticeTomáš KrajíčekОценок пока нет
- Blinding: Linking Evidence To PracticeДокумент2 страницыBlinding: Linking Evidence To PracticeTomáš KrajíčekОценок пока нет
- Control Groups: Linking Evidence To PracticeДокумент2 страницыControl Groups: Linking Evidence To PracticeTomáš KrajíčekОценок пока нет
- Engaging With Research: Linking Evidence With PracticeДокумент2 страницыEngaging With Research: Linking Evidence With PracticeTomáš KrajíčekОценок пока нет
- Gufoni Maneuver: Horizontal Canal BPPVДокумент19 страницGufoni Maneuver: Horizontal Canal BPPVTomáš KrajíčekОценок пока нет
- Particle FilterДокумент16 страницParticle Filterlevin696Оценок пока нет
- Acid Bases and Salts Previous Year Questiosn Class 10 ScienceДокумент5 страницAcid Bases and Salts Previous Year Questiosn Class 10 Scienceclashhunting123123Оценок пока нет
- Reducing Motor Vehicle Crashes in B.C.Документ260 страницReducing Motor Vehicle Crashes in B.C.Jeff NagelОценок пока нет
- Small Scale IndustriesДокумент6 страницSmall Scale IndustriesMangesh KadamОценок пока нет
- Food Product Innovation PDFДокумент35 страницFood Product Innovation PDFDidik HariadiОценок пока нет
- Science 10 FINAL Review 2014Документ49 страницScience 10 FINAL Review 2014Zara Zalaal [Student]Оценок пока нет
- Legal Aspects of Construction Ethics PaperДокумент11 страницLegal Aspects of Construction Ethics PaperbikaresОценок пока нет
- EASA CS-22 Certification of SailplanesДокумент120 страницEASA CS-22 Certification of SailplanessnorrigОценок пока нет
- Japanese Mythology: 2 Kuniumi and KamiumiДокумент12 страницJapanese Mythology: 2 Kuniumi and KamiumipdekraaijОценок пока нет
- BIO SCI OsmosisДокумент10 страницBIO SCI OsmosisJoy FernandezОценок пока нет
- DrosteДокумент4 страницыDrosteapi-478100074Оценок пока нет
- FTP Booster Training Plan OverviewДокумент1 страницаFTP Booster Training Plan Overviewwiligton oswaldo uribe rodriguezОценок пока нет
- AVR On Load Tap ChangerДокумент39 страницAVR On Load Tap ChangerInsan Aziz100% (1)
- Ecological Building: Term Project For ME 599Документ32 страницыEcological Building: Term Project For ME 599Junaid AnwarОценок пока нет
- Seminar ReportДокумент15 страницSeminar ReportNipesh MAHARJANОценок пока нет
- Lab5.ipynb - ColaboratoryДокумент8 страницLab5.ipynb - ColaboratoryMin YОценок пока нет
- 44Документ2 страницы44menakadevieceОценок пока нет
- RTOS6Документ20 страницRTOS6Krishna ChaitanyaОценок пока нет
- Chen Probable Cause Affidavit 050714Документ7 страницChen Probable Cause Affidavit 050714USA TODAYОценок пока нет
- Microtech Testing & Research Laboratory: Condition of Sample, When Received: SatisfactoryДокумент1 страницаMicrotech Testing & Research Laboratory: Condition of Sample, When Received: SatisfactoryKumar AbhishekОценок пока нет
- R820T Datasheet-Non R-20111130 UnlockedДокумент26 страницR820T Datasheet-Non R-20111130 UnlockedKonstantinos GoniadisОценок пока нет
- Prepared by M Suresh Kumar, Chief Manager Faculty, SBILD HYDERABADДокумент29 страницPrepared by M Suresh Kumar, Chief Manager Faculty, SBILD HYDERABADBino JosephОценок пока нет
- A Randomised Clinical Trial Comparing Myoinositol and Metformin in PCOSДокумент7 страницA Randomised Clinical Trial Comparing Myoinositol and Metformin in PCOSAtika NajlaОценок пока нет
- CH 11 International TradeДокумент20 страницCH 11 International TradeSANTU GHORAIОценок пока нет
- Block 7Документ62 страницыBlock 7Poco ChanОценок пока нет
- EmbOS GenericДокумент324 страницыEmbOS Genericbogd33Оценок пока нет
- Richard Dennis Sonterra Capital Vs Cba Nab Anz Macquarie Gov - Uscourts.nysd.461685.1.0-1Документ87 страницRichard Dennis Sonterra Capital Vs Cba Nab Anz Macquarie Gov - Uscourts.nysd.461685.1.0-1Maverick MinitriesОценок пока нет
- Hypertension ESC 2013 PDFДокумент32 страницыHypertension ESC 2013 PDFNar RungrojanarakОценок пока нет