Вам также может понравиться
- Powerpoint Presentation R.A 7877 - Anti Sexual Harassment ActДокумент14 страницPowerpoint Presentation R.A 7877 - Anti Sexual Harassment ActApple100% (1)
- Conflict WaiverДокумент2 страницыConflict WaiverjlurosОценок пока нет
- Maternal Death ReviewsДокумент4 страницыMaternal Death ReviewsJosephine AikpitanyiОценок пока нет
- Practitioners Guide For Business Development Planning in FPOsДокумент70 страницPractitioners Guide For Business Development Planning in FPOsMythreyi ChichulaОценок пока нет
- Chapter Two Complexity AnalysisДокумент40 страницChapter Two Complexity AnalysisSoressa HassenОценок пока нет
- Mercury 150HPДокумент5 страницMercury 150HP이영석0% (1)
- MEMORANDUMДокумент8 страницMEMORANDUMAdee JocsonОценок пока нет
- Home Guaranty Corp. v. Manlapaz - PunzalanДокумент3 страницыHome Guaranty Corp. v. Manlapaz - PunzalanPrincess Aliyah Punzalan100% (1)
- Data-Driven Healthcare: Revolutionizing Patient Care with Data ScienceОт EverandData-Driven Healthcare: Revolutionizing Patient Care with Data ScienceОценок пока нет
- Delta PresentationДокумент36 страницDelta Presentationarch_ianОценок пока нет
- To Err Is Human 1999 Report Brief PDFДокумент8 страницTo Err Is Human 1999 Report Brief PDFAjib A. Azis100% (3)
- Managerial Accounting-Fundamental Concepts and Costing Systems For Cost Analysis Module 1Документ40 страницManagerial Accounting-Fundamental Concepts and Costing Systems For Cost Analysis Module 1Uzma Khan100% (1)
- Rehabilitation and Retrofitting of Structurs Question PapersДокумент4 страницыRehabilitation and Retrofitting of Structurs Question PapersYaswanthGorantlaОценок пока нет
- Nursing Ethical Dilemma With Using Informatics Technology: March 2019Документ10 страницNursing Ethical Dilemma With Using Informatics Technology: March 2019Ahmed MasoudОценок пока нет
- Respectful Maternity Care: An Overview PowerpointДокумент15 страницRespectful Maternity Care: An Overview PowerpointJhpiego100% (1)
- Perceived Safety Culture of Healthcare Providers in Hospitals in The PhilippinesДокумент14 страницPerceived Safety Culture of Healthcare Providers in Hospitals in The PhilippinesRhod Bernaldez EstaОценок пока нет
- Research Papers On Access To HealthcareДокумент7 страницResearch Papers On Access To Healthcaregw1w9reg100% (1)
- A Global Database of Abortion Laws, Policies, Health Standards and GuidelinesДокумент6 страницA Global Database of Abortion Laws, Policies, Health Standards and GuidelinesRahmadani NabilaОценок пока нет
- Optimising Caesarean Section Use 3: Interventions To Reduce Unnecessary Caesarean Sections in Healthy Women and BabiesДокумент11 страницOptimising Caesarean Section Use 3: Interventions To Reduce Unnecessary Caesarean Sections in Healthy Women and Babiesforensik24mei koasdaringОценок пока нет
- Ethical Concerns Relating To Taking Birth Control PillsДокумент8 страницEthical Concerns Relating To Taking Birth Control PillsMichael MbithiОценок пока нет
- Abortion ResearchДокумент56 страницAbortion Researchcodmluna3Оценок пока нет
- The Applications of Mobile Health Technology (Mhealth) in Reducing Maternal Mortality and Improving Maternal Health - Sarah KimДокумент16 страницThe Applications of Mobile Health Technology (Mhealth) in Reducing Maternal Mortality and Improving Maternal Health - Sarah KimnurjОценок пока нет
- Workshop MigHealthCare StrengtheningДокумент1 страницаWorkshop MigHealthCare StrengtheningYang GuoОценок пока нет
- Criteria Possible Points Points EarnedДокумент6 страницCriteria Possible Points Points Earnedapi-350882100Оценок пока нет
- Ethical Aspects of Digital Health From A Justice Point of ViewДокумент5 страницEthical Aspects of Digital Health From A Justice Point of ViewAlejo DavidОценок пока нет
- Framework For Ensuring Human Rights in The Provision of Contraceptive Information and ServicesДокумент24 страницыFramework For Ensuring Human Rights in The Provision of Contraceptive Information and ServicesSara Fernandez RiveraОценок пока нет
- Articulo Publicado Frontiers Public HealthДокумент17 страницArticulo Publicado Frontiers Public HealthKathia Cancino RojasОценок пока нет
- 1-Teen Pregnancy As A Public Health Problem.....Документ6 страниц1-Teen Pregnancy As A Public Health Problem.....catholic HymnsОценок пока нет
- 5139 BC 262Документ7 страниц5139 BC 262wowlwowlskeowОценок пока нет
- Disease Control Priority-3Документ23 страницыDisease Control Priority-3Abubakar Abdhoo100% (1)
- Nurses and Health Professionals Facing Female GeniДокумент12 страницNurses and Health Professionals Facing Female GeniBiaОценок пока нет
- Mapeh 10Документ17 страницMapeh 10mary triskayeОценок пока нет
- WYA Reproductive Health White PaperДокумент20 страницWYA Reproductive Health White PaperWorld Youth AllianceОценок пока нет
- Global Abortion Policies DatabaseДокумент5 страницGlobal Abortion Policies DatabaseHumberto Herrera GutierrezОценок пока нет
- Ethics, Privacy, and SecurityДокумент10 страницEthics, Privacy, and SecuritySittie Aina Munder100% (1)
- Ryzza BaldiviesoДокумент31 страницаRyzza BaldiviesoRobert DemagneОценок пока нет
- Moving Beyond Disrespect and Abuse Addressing The Structural Dimensions of Obstetric VioleДокумент10 страницMoving Beyond Disrespect and Abuse Addressing The Structural Dimensions of Obstetric VioleMaryОценок пока нет
- A Review of Women's Intellectual Contribution Under The Bureaucracy in PakistanДокумент36 страницA Review of Women's Intellectual Contribution Under The Bureaucracy in PakistansalmankhataniОценок пока нет
- Research PartialДокумент8 страницResearch PartialAmie VОценок пока нет
- GP ScaffoldДокумент7 страницGP ScaffoldMinh HoangОценок пока нет
- Torts Research Paper 1Документ8 страницTorts Research Paper 1Cristelle Estrada-Romuar JurolanОценок пока нет
- What Is Health Informatics?Документ4 страницыWhat Is Health Informatics?Yna HerraduraОценок пока нет
- Main Content JuryДокумент15 страницMain Content Juryarushi.singhОценок пока нет
- WHO Recommendations On Antenatal Care For A Positive Pregnancy Experience in KenyaДокумент10 страницWHO Recommendations On Antenatal Care For A Positive Pregnancy Experience in KenyaMartin Otundo RichardОценок пока нет
- The Safe Motherhood InitiativeДокумент3 страницыThe Safe Motherhood InitiativeAnonymous g6L7jJWОценок пока нет
- ResearchProposal FinalDraft MirandaDuckworthДокумент13 страницResearchProposal FinalDraft MirandaDuckworthMiranda DuckworthОценок пока нет
- Jurnal 1Документ10 страницJurnal 1dinidinayОценок пока нет
- Association of Rule of Law and Health Outcomes: An Ecological StudyДокумент9 страницAssociation of Rule of Law and Health Outcomes: An Ecological StudybogdanОценок пока нет
- Uu200 EthicsДокумент6 страницUu200 EthicsFiza AliОценок пока нет
- World Health Organization: by Wendy BraunДокумент8 страницWorld Health Organization: by Wendy BraunAnonymous AvbmJ5JTОценок пока нет
- Debating Medicalization of Female Genital Mutilation/Cutting (FGM/C) : Learning From (Policy) Experiences Across CountriesДокумент10 страницDebating Medicalization of Female Genital Mutilation/Cutting (FGM/C) : Learning From (Policy) Experiences Across CountriesPutu AdiОценок пока нет
- Child Sexual Abuse: Current Evidence, Clinical Practice, and Policy DirectionsОт EverandChild Sexual Abuse: Current Evidence, Clinical Practice, and Policy DirectionsОценок пока нет
- Evaluation of The Effect of Birth and Death Registration On Health Service Delivery (A Case of Tolon District of Ghana)Документ10 страницEvaluation of The Effect of Birth and Death Registration On Health Service Delivery (A Case of Tolon District of Ghana)Igbani VictoryОценок пока нет
- Kesehatan Anak (Child Health)Документ15 страницKesehatan Anak (Child Health)AndiniОценок пока нет
- WHO Coșbuc MUN 2023 Study GuideДокумент17 страницWHO Coșbuc MUN 2023 Study Guideluca mscОценок пока нет
- Ryzza - Baldivieso 2Документ34 страницыRyzza - Baldivieso 2Robert DemagneОценок пока нет
- Ensuring The Accessibility of Standard Health Care System and Reproductive Rights For Pregnant Women and Children Amid Covid-19 Pandemic. OverviewДокумент9 страницEnsuring The Accessibility of Standard Health Care System and Reproductive Rights For Pregnant Women and Children Amid Covid-19 Pandemic. Overviewaxium 2014Оценок пока нет
- Lecture 1intro RHДокумент32 страницыLecture 1intro RHAd Nan AbduselamОценок пока нет
- JournalДокумент2 страницыJournalRenalyn MangadchilОценок пока нет
- Jurnal Jaminan KesДокумент25 страницJurnal Jaminan KesMeisya MonicaОценок пока нет
- Maternal Mortality PDFДокумент101 страницаMaternal Mortality PDFCamille Joy BaliliОценок пока нет
- JHJHJJHДокумент14 страницJHJHJJHnur arifahОценок пока нет
- PR1 RRLДокумент4 страницыPR1 RRLalayanjoshua26Оценок пока нет
- Reproductive and Child Health ProgrammeДокумент2 страницыReproductive and Child Health ProgrammeAnnapurna DangetiОценок пока нет
- Public Health Delivery in The Information Age - The Role of Informatics and TechnologyДокумент22 страницыPublic Health Delivery in The Information Age - The Role of Informatics and Technologysbaracaldo2Оценок пока нет
- Disaster Nursing Final ModuleДокумент7 страницDisaster Nursing Final ModuleJerome Reyes is PogiОценок пока нет
- Aismun 2020 - Un Women Committee GuideДокумент29 страницAismun 2020 - Un Women Committee GuideLauraОценок пока нет
- Incident Reporting SystemsДокумент5 страницIncident Reporting SystemsPaulo'RodriguesОценок пока нет
- Pharm Info Lab PrefiДокумент1 страницаPharm Info Lab PreficalopemichelleОценок пока нет
- Literature Review On Neonatal DeathДокумент6 страницLiterature Review On Neonatal Deathafdtovmhb100% (1)
- FNCP GroupДокумент13 страницFNCP GroupTanya PinedaОценок пока нет
- Public Health Laws Affecting The Practice of Nursing PDFДокумент118 страницPublic Health Laws Affecting The Practice of Nursing PDFTanya PinedaОценок пока нет
- NutriiiДокумент1 страницаNutriiiTanya PinedaОценок пока нет
- Table Synthesis ContextДокумент2 страницыTable Synthesis ContextTanya PinedaОценок пока нет
- Literatur Matrix NCM RleДокумент3 страницыLiteratur Matrix NCM RleTanya PinedaОценок пока нет
- Defeating An Old Adversary Cement Kiln BallsДокумент5 страницDefeating An Old Adversary Cement Kiln BallsManish KumarОценок пока нет
- STM Series Solar ControllerДокумент2 страницыSTM Series Solar ControllerFaris KedirОценок пока нет
- Terms and Conditions 27 06 PDFДокумент4 страницыTerms and Conditions 27 06 PDFShreyash NaikwadiОценок пока нет
- Bank of AmericaДокумент1 страницаBank of AmericaBethany MangahasОценок пока нет
- Sign Language To Speech ConversionДокумент6 страницSign Language To Speech ConversionGokul RajaОценок пока нет
- 7Документ101 страница7Navindra JaggernauthОценок пока нет
- Creative Thinking (2) : Dr. Sarah Elsayed ElshazlyДокумент38 страницCreative Thinking (2) : Dr. Sarah Elsayed ElshazlyNehal AbdellatifОценок пока нет
- Salem Telephone CompanyДокумент4 страницыSalem Telephone Company202211021 imtnagОценок пока нет
- Health, Safety & Environment: Refer NumberДокумент2 страницыHealth, Safety & Environment: Refer NumbergilОценок пока нет
- Circuitos Digitales III: #IncludeДокумент2 страницыCircuitos Digitales III: #IncludeCristiamОценок пока нет
- Pthread TutorialДокумент26 страницPthread Tutorialapi-3754827Оценок пока нет
- Income Tax Calculator 2023Документ50 страницIncome Tax Calculator 2023TARUN PRASADОценок пока нет
- Practical GAD (1-32) Roll No.20IF227Документ97 страницPractical GAD (1-32) Roll No.20IF22720IF135 Anant PatilОценок пока нет
- Is.14785.2000 - Coast Down Test PDFДокумент12 страницIs.14785.2000 - Coast Down Test PDFVenkata NarayanaОценок пока нет
- Simavi - Project Officer PROPOPIДокумент4 страницыSimavi - Project Officer PROPOPIAgus NugrahaОценок пока нет
- Kompetensi Sumber Daya Manusia SDM Dalam Meningkatkan Kinerja Tenaga Kependidika PDFДокумент13 страницKompetensi Sumber Daya Manusia SDM Dalam Meningkatkan Kinerja Tenaga Kependidika PDFEka IdrisОценок пока нет
- Question Bank For Vlsi LabДокумент4 страницыQuestion Bank For Vlsi LabSav ThaОценок пока нет
- Tate Modern London, Pay Congestion ChargeДокумент6 страницTate Modern London, Pay Congestion ChargeCongestionChargeОценок пока нет
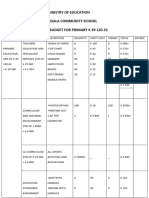
- Ministry of Education Musala SCHДокумент5 страницMinistry of Education Musala SCHlaonimosesОценок пока нет