Вам также может понравиться
- Pathology of Female Cancers: Precursor and Early-Stage Breast, Ovarian and Uterine CarcinomasОт EverandPathology of Female Cancers: Precursor and Early-Stage Breast, Ovarian and Uterine CarcinomasTakuya MoriyaОценок пока нет
- Pi Is 0002937811009379Документ9 страницPi Is 0002937811009379Mirza FinandarОценок пока нет
- Absolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationОт EverandAbsolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationОценок пока нет
- Placenta Accreta A Practical Review 2020Документ6 страницPlacenta Accreta A Practical Review 2020Adriana MartínezОценок пока нет
- Manajemen Plasent AkretaДокумент14 страницManajemen Plasent AkretaangelОценок пока нет
- Jurnal Obgyn 2018 2Документ15 страницJurnal Obgyn 2018 2aulОценок пока нет
- Jurnal 2018Документ9 страницJurnal 2018aulОценок пока нет
- Acute Uterine InversionДокумент6 страницAcute Uterine InversionBima GhovaroliyОценок пока нет
- Placenta Accreta Spectrum Disorders: Challenges, Risks, and Management StrategiesДокумент13 страницPlacenta Accreta Spectrum Disorders: Challenges, Risks, and Management StrategiesRahmayantiYuliaОценок пока нет
- Acute Inversion of The Uterus PDFДокумент6 страницAcute Inversion of The Uterus PDFEvelyn TingОценок пока нет
- Obstetrics V10 Common Obstetric Conditions Chapter Placenta Previa and Placenta Abruption 1665345717Документ17 страницObstetrics V10 Common Obstetric Conditions Chapter Placenta Previa and Placenta Abruption 1665345717Mauricio Lopez MejiaОценок пока нет
- BJMG 20 005 PDFДокумент5 страницBJMG 20 005 PDFRakka Fawwaz IlhamОценок пока нет
- Society For Maternal-Fetal Medicine (SMFM) Consult Series #49: Cesarean Scar PregnancyДокумент13 страницSociety For Maternal-Fetal Medicine (SMFM) Consult Series #49: Cesarean Scar PregnancyTandyo TriasmoroОценок пока нет
- 2 Pamj-33-86Документ12 страниц2 Pamj-33-86arumОценок пока нет
- Sutura CesareasДокумент10 страницSutura CesareasalexОценок пока нет
- Ectopico en Cicatriz de Cesarea, 2022Документ12 страницEctopico en Cicatriz de Cesarea, 2022rafael martinezОценок пока нет
- Frequency of Morbidly Adherent Placenta in Previous Scar: Fakhar Un Nissa, Saira Dars, Shazia Awan, Firdous MumtazДокумент5 страницFrequency of Morbidly Adherent Placenta in Previous Scar: Fakhar Un Nissa, Saira Dars, Shazia Awan, Firdous MumtazprobouОценок пока нет
- Conservative Manangement v2.BS - LSДокумент27 страницConservative Manangement v2.BS - LSOihane Manterola LasaОценок пока нет
- Placenta Previa, Accreta, & Vasa Previa 2006Документ15 страницPlacenta Previa, Accreta, & Vasa Previa 2006Ika Agustin0% (1)
- Obstetricia Iii Placenta AcretaДокумент22 страницыObstetricia Iii Placenta AcretaHugo GutiérrezОценок пока нет
- Placenta Accreta Spectrum and Postpartum Hemorrhag - 230510 - 170158Документ10 страницPlacenta Accreta Spectrum and Postpartum Hemorrhag - 230510 - 170158Nilfacio PradoОценок пока нет
- Committee Opinion: Placenta AccretaДокумент5 страницCommittee Opinion: Placenta AccretaagungОценок пока нет
- Jurnal Plasenta Akreta PDFДокумент5 страницJurnal Plasenta Akreta PDFfatqur28Оценок пока нет
- The Placenta Accreta Spectrum: Pathophysiology and Evidence-Based Anatomy For Prenatal Ultrasound ImagingДокумент14 страницThe Placenta Accreta Spectrum: Pathophysiology and Evidence-Based Anatomy For Prenatal Ultrasound ImagingIriamana Liasyarah MarudinОценок пока нет
- Placenta Acreta SpectrumДокумент50 страницPlacenta Acreta Spectrum6ixSideCreate MОценок пока нет
- Placenta Previa PDFДокумент15 страницPlacenta Previa PDFDamaris GonzálezОценок пока нет
- Managing Placenta Accreta: Incidence and PathophysiologyДокумент9 страницManaging Placenta Accreta: Incidence and PathophysiologyAslesa Wangpathi PagehgiriОценок пока нет
- Artículo Redalyc 323449162009Документ10 страницArtículo Redalyc 323449162009DesyHandayaniОценок пока нет
- Committee Opinion: Placenta AccretaДокумент5 страницCommittee Opinion: Placenta AccretabebetteryesyoucanОценок пока нет
- Screening For Placenta Accreta at 11-14 Weeks of GestationДокумент6 страницScreening For Placenta Accreta at 11-14 Weeks of Gestationjuljim01Оценок пока нет
- Article 262063-PrintДокумент15 страницArticle 262063-PrintAhsan AuliyaОценок пока нет
- 11 Abnormal PlacentationДокумент29 страниц11 Abnormal PlacentationMaria Gabriela CristanchoОценок пока нет
- Hemorragia y EmbrazoДокумент6 страницHemorragia y Embrazoana catalinaОценок пока нет
- Silver 2015Документ15 страницSilver 2015Farlinda AlyaОценок пока нет
- Articulo 8Документ15 страницArticulo 8Monica ReyesОценок пока нет
- Incidence and Risk Factors For Placenta Accreta/Increta/ Percreta in The UK: A National Case-Control StudyДокумент6 страницIncidence and Risk Factors For Placenta Accreta/Increta/ Percreta in The UK: A National Case-Control StudyRahmayantiYuliaОценок пока нет
- Background: Placenta Previa. Placenta Previa Covering The Entire CervicalДокумент9 страницBackground: Placenta Previa. Placenta Previa Covering The Entire CervicalOkto Sofyan HasanОценок пока нет
- Moxibustion To Correct A Breech Presentation of The Fetus Author IDEASSДокумент13 страницMoxibustion To Correct A Breech Presentation of The Fetus Author IDEASSVraciul din VeciniОценок пока нет
- Hemorragia Placenta PreviaДокумент8 страницHemorragia Placenta PreviaAngel BerardiОценок пока нет
- PIIS0015028219304844Документ2 страницыPIIS0015028219304844nighshift serialsleeperОценок пока нет
- Diagnosis and Management of Isthmocele (Cesarean Scar Defect) A SWOT AnalysisДокумент9 страницDiagnosis and Management of Isthmocele (Cesarean Scar Defect) A SWOT AnalysisWillans Eduardo Rosha HumerezОценок пока нет
- Type and Location of Placenta Previa Affect Preterm Delivery Risk Related To Antepartum HemorrhageДокумент7 страницType and Location of Placenta Previa Affect Preterm Delivery Risk Related To Antepartum HemorrhageBuya TaftaОценок пока нет
- Caesareans Section Scar Ectopic Pregnancy: An Emerging ChallengeДокумент24 страницыCaesareans Section Scar Ectopic Pregnancy: An Emerging Challengenighshift serialsleeperОценок пока нет
- Maternal and FДокумент3 страницыMaternal and FNununkОценок пока нет
- The New World of Placenta Accreta Spectrum Disorders: Special EditorialДокумент2 страницыThe New World of Placenta Accreta Spectrum Disorders: Special EditorialNahrisyah Ulfa SafnaОценок пока нет
- Partus LamaДокумент11 страницPartus LamaSulis SipinОценок пока нет
- Literature Review Placenta PreviaДокумент7 страницLiterature Review Placenta Previaeygyabvkg100% (2)
- Pesario - SMFMДокумент3 страницыPesario - SMFMDaniela Franco HОценок пока нет
- Placental Abnormalities: Placenta Accreta, Placenta Increta, and Placenta PercretaДокумент11 страницPlacental Abnormalities: Placenta Accreta, Placenta Increta, and Placenta PercretaLiza M. PurocОценок пока нет
- Cme Reviewarticle: Assessing Cephalopelvic Disproportion: Back To The BasicsДокумент9 страницCme Reviewarticle: Assessing Cephalopelvic Disproportion: Back To The BasicsvickyОценок пока нет
- Placenta Accreta Spectrum Into The Parametrium Morbidity Differences Between Upper and Lower LocationДокумент8 страницPlacenta Accreta Spectrum Into The Parametrium Morbidity Differences Between Upper and Lower Locationmar.garciaОценок пока нет
- The Application of The Management Protocol of Invasive Placenta. A Case ReportДокумент5 страницThe Application of The Management Protocol of Invasive Placenta. A Case ReportFlorina PaulaОценок пока нет
- PlacentaДокумент17 страницPlacentarizka auliaОценок пока нет
- Homepage: - : IntroductionДокумент7 страницHomepage: - : IntroductionIJAR JOURNALОценок пока нет
- Maternal and Fetal Outcome in Placenta Accreta Spectrum (PAS) Associated With Placenta Previa: A Retrospective Analysis From A Tertiary CenterДокумент9 страницMaternal and Fetal Outcome in Placenta Accreta Spectrum (PAS) Associated With Placenta Previa: A Retrospective Analysis From A Tertiary CenterwindawaahhОценок пока нет
- Caesarean Scar Pregnancy. Diagnosis, Natural History and Treatment (Curr Opin Obstet Gynecol - Oct 2022)Документ8 страницCaesarean Scar Pregnancy. Diagnosis, Natural History and Treatment (Curr Opin Obstet Gynecol - Oct 2022)garomeros5366Оценок пока нет
- To Ignore or Not To Ignore Placental Calcifications On Prenatal Ultrasound: A Systematic Review and Meta-AnalysisДокумент22 страницыTo Ignore or Not To Ignore Placental Calcifications On Prenatal Ultrasound: A Systematic Review and Meta-AnalysisMaulida HalimahОценок пока нет
- Placenta Previa: ObjectivesДокумент6 страницPlacenta Previa: ObjectivesAllan Lyndon LariosОценок пока нет
- Case Study AccretaДокумент35 страницCase Study AccretaM Clarisse ParicoОценок пока нет
- Refractory Uterine Atony-Still A Problem After All These YearsДокумент9 страницRefractory Uterine Atony-Still A Problem After All These YearsIndah 15Оценок пока нет
- 1998 Volvo s70-v70Документ52 страницы1998 Volvo s70-v70Raul DoctoОценок пока нет
- Seminar: Jan Claassen, Soojin ParkДокумент17 страницSeminar: Jan Claassen, Soojin ParkRaul DoctoОценок пока нет
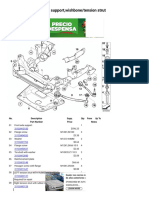
- X3 E83 X3 3.0i FRNT Axle Support, Wishbone Tension StrutДокумент3 страницыX3 E83 X3 3.0i FRNT Axle Support, Wishbone Tension StrutRaul DoctoОценок пока нет
- BMW 6 Cylinder Dual Vanos Piston Seal Repair Fix PДокумент13 страницBMW 6 Cylinder Dual Vanos Piston Seal Repair Fix PRaul DoctoОценок пока нет
- Central Venous Pressure (CVP)Документ3 страницыCentral Venous Pressure (CVP)Raul DoctoОценок пока нет
- Ascoping Review of The Pathophysiology of COVID-19Документ16 страницAscoping Review of The Pathophysiology of COVID-19Raul DoctoОценок пока нет
- An Update On COVID-19 and Pregnancy: Djamieson@emory - EduДокумент10 страницAn Update On COVID-19 and Pregnancy: Djamieson@emory - EduRaul DoctoОценок пока нет
- Vlaar2021 Article TransfusionStrategiesInBleedinДокумент25 страницVlaar2021 Article TransfusionStrategiesInBleedinRaul DoctoОценок пока нет
- Why Exercise Builds Muscles: Titin Mechanosensing Controls Skeletal Muscle Growth Under LoadДокумент15 страницWhy Exercise Builds Muscles: Titin Mechanosensing Controls Skeletal Muscle Growth Under LoadRaul Docto100% (1)
- 2022 ACC A-Ha HFSAGuideline For The Management of Heart FailureДокумент167 страниц2022 ACC A-Ha HFSAGuideline For The Management of Heart FailureRaul DoctoОценок пока нет
- Obstetrics & GynecologyДокумент10 страницObstetrics & GynecologyRaul DoctoОценок пока нет
- How To Install Google Play On The Amazon Fire HD 8Документ7 страницHow To Install Google Play On The Amazon Fire HD 8Raul DoctoОценок пока нет
- Case 35-2021: A 50-Year-Old Woman With Pain in The Left Upper Quadrant and HypoxemiaДокумент7 страницCase 35-2021: A 50-Year-Old Woman With Pain in The Left Upper Quadrant and HypoxemiaRaul DoctoОценок пока нет
- Tugwell 1985Документ13 страницTugwell 1985Raul DoctoОценок пока нет
- Human Infection With Strongyloides Stercoralis and Other Related Strongyloides SpeciesДокумент11 страницHuman Infection With Strongyloides Stercoralis and Other Related Strongyloides SpeciesRaul DoctoОценок пока нет
- 007 Obgyn-CatalogДокумент100 страниц007 Obgyn-CatalogRaul DoctoОценок пока нет
- Heparin Resistance - Clinical Perspectives and Management StrategiesДокумент7 страницHeparin Resistance - Clinical Perspectives and Management StrategiesRaul DoctoОценок пока нет
- Author 'S Accepted ManuscriptДокумент46 страницAuthor 'S Accepted ManuscriptRaul DoctoОценок пока нет
- Ventilator Weaning and Spontaneous Breathing Trials An Educational ReviewДокумент7 страницVentilator Weaning and Spontaneous Breathing Trials An Educational ReviewRaul DoctoОценок пока нет
- Lecture 1: NeuroembryologyДокумент13 страницLecture 1: NeuroembryologyRaul DoctoОценок пока нет
- Prolonged Pregnancy:When Should We Intervene?Документ11 страницProlonged Pregnancy:When Should We Intervene?Raul DoctoОценок пока нет
- Management Review Meeting SampleДокумент12 страницManagement Review Meeting SampleTalibah Seeker After Knowlegde100% (1)
- A Study On Burnout of Nurses in The Period of COVID-19Документ6 страницA Study On Burnout of Nurses in The Period of COVID-19OsamaОценок пока нет
- Research PaperДокумент10 страницResearch PaperAyyat FatimaОценок пока нет
- Fundamentals of NursingДокумент268 страницFundamentals of Nursinguhta100% (1)
- Sexual Reproductive Health Program FGM and Child Early/Forced Marriage (FGM and CEFM) ProjectДокумент4 страницыSexual Reproductive Health Program FGM and Child Early/Forced Marriage (FGM and CEFM) ProjectOmar Hassen100% (1)
- Community Health Nursing Approach: Mrs - Neethu Vincent Asst Professor KVM College of NursingДокумент21 страницаCommunity Health Nursing Approach: Mrs - Neethu Vincent Asst Professor KVM College of NursingNeethu VincentОценок пока нет
- Magnet TherapyДокумент10 страницMagnet TherapyMarvick Chuquiruna ChavezОценок пока нет
- Forgiveness-Test QuestionsДокумент2 страницыForgiveness-Test QuestionspbpdsОценок пока нет
- Community Nursing Skill and CompetenceДокумент54 страницыCommunity Nursing Skill and CompetenceHeri Zalmes Dodge TomahawkОценок пока нет
- HIV - LancetДокумент13 страницHIV - LancetcristhianldsОценок пока нет
- Exploring TheДокумент20 страницExploring TheMiroslava DjordjevicОценок пока нет
- Tourist Safety and SecurityДокумент166 страницTourist Safety and SecurityGiancarlo Gallegos Peralta100% (1)
- BBLK Surabaya: National Tuberculosis Reference Laboratory For Culture/Drug Susceptibility TestingДокумент12 страницBBLK Surabaya: National Tuberculosis Reference Laboratory For Culture/Drug Susceptibility TestingMas Paijo PeloukОценок пока нет
- Department of Education: Republic of The PhilippinesДокумент8 страницDepartment of Education: Republic of The PhilippinesReysa m. DuatinОценок пока нет
- Science EssayДокумент2 страницыScience EssayRehoboth EljakyОценок пока нет
- Resume O4 Lydm Edmonton AutosavedДокумент3 страницыResume O4 Lydm Edmonton Autosavedapi-314849412Оценок пока нет
- Cervicogenic Tension-Type Migraine Cluster Occipital Neuralgia Cause LocationДокумент1 страницаCervicogenic Tension-Type Migraine Cluster Occipital Neuralgia Cause LocationAlpacaОценок пока нет
- Civil Liberties and Civil Commitment: The Therapeutic State by Thomas SzaszДокумент2 страницыCivil Liberties and Civil Commitment: The Therapeutic State by Thomas SzaszAbdelrahman Abdallah TI from London RIPОценок пока нет
- The Children Act 1989 Guidance and RegulationДокумент186 страницThe Children Act 1989 Guidance and RegulationkvisaОценок пока нет
- Acute Herpetic Gingivostomatitis Associated With Herpes Simplex Virus 2Документ4 страницыAcute Herpetic Gingivostomatitis Associated With Herpes Simplex Virus 2Ayu KartikaОценок пока нет
- Acetylcysteine 200mg (Siran, Reolin)Документ5 страницAcetylcysteine 200mg (Siran, Reolin)ddandan_2Оценок пока нет
- Consultation and Liaison Consultation and Liaison Psychiatry (PDFDrive)Документ70 страницConsultation and Liaison Consultation and Liaison Psychiatry (PDFDrive)mlll100% (1)
- Cheryl Updated Resume 372013Документ2 страницыCheryl Updated Resume 372013api-245086462Оценок пока нет
- Ventricular Aneurysm: PathophysiologyДокумент3 страницыVentricular Aneurysm: PathophysiologyMegan N. ReyesОценок пока нет
- What Is Dietary Fiber? Benefits of FiberДокумент4 страницыWhat Is Dietary Fiber? Benefits of Fiberjonabelle eranОценок пока нет
- Entamoeba HistolyticaДокумент6 страницEntamoeba HistolyticaWan Nur AnisaОценок пока нет
- Certificate IV in Commercial Cookery Sit 40516Документ8 страницCertificate IV in Commercial Cookery Sit 40516Tikaram GhimireОценок пока нет
- Tata Laksana Konseling GiziДокумент9 страницTata Laksana Konseling GiziJeannete Claudia WulandariОценок пока нет
- OET Practice Reading Test Part A:: JourneyДокумент9 страницOET Practice Reading Test Part A:: JourneyPrasoon PremrajОценок пока нет
- Physical Examination ScoliosisДокумент7 страницPhysical Examination Scoliosisyosua_edwinОценок пока нет
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Рейтинг: 3 из 5 звезд3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 4.5 из 5 звезд4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesОт EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesРейтинг: 4.5 из 5 звезд4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 4 из 5 звезд4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4.5 из 5 звезд4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceОт EverandTo Explain the World: The Discovery of Modern ScienceРейтинг: 3.5 из 5 звезд3.5/5 (51)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsОт EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsРейтинг: 4.5 из 5 звезд4.5/5 (39)
- The Marshmallow Test: Mastering Self-ControlОт EverandThe Marshmallow Test: Mastering Self-ControlРейтинг: 4.5 из 5 звезд4.5/5 (60)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingОт EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingРейтинг: 4 из 5 звезд4/5 (1138)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)