Вам также может понравиться
- AssignmentДокумент8 страницAssignmentMarijo DolojolОценок пока нет
- Diagnostic Evaluation in Respiratory Conditions-1Документ68 страницDiagnostic Evaluation in Respiratory Conditions-1pashiem88Оценок пока нет
- Roles of Bone Marrow Transplant Unit Nurses IncludesДокумент10 страницRoles of Bone Marrow Transplant Unit Nurses IncludesGleden UmayamОценок пока нет
- Placenta PreviaДокумент54 страницыPlacenta PreviabobtagubaОценок пока нет
- Evaluation ReviewДокумент11 страницEvaluation Reviewviwoyir626Оценок пока нет
- Cesarean Section & Tubal Ligation SurgeryДокумент16 страницCesarean Section & Tubal Ligation SurgerySteffiОценок пока нет
- Evaluation ReviewДокумент11 страницEvaluation Reviewviwoyir626Оценок пока нет
- Icu Protocols-1Документ38 страницIcu Protocols-1M.IMRAN ANJUM100% (1)
- Ats PR Assembly Re Opening PR Document FinalДокумент8 страницAts PR Assembly Re Opening PR Document FinalElliot AndersonОценок пока нет
- CT Scanpatient PreparationДокумент20 страницCT Scanpatient PreparationJohn Paul MarasiganОценок пока нет
- Clinician Pocket GuideДокумент2 страницыClinician Pocket Guideroxy357Оценок пока нет
- Policies and Procedures Radiology DepartmentДокумент6 страницPolicies and Procedures Radiology DepartmentRalph Gerard Saldajeno ValdespinaОценок пока нет
- Group 2 - Rose & Sadava - VATSДокумент23 страницыGroup 2 - Rose & Sadava - VATSRay Anthony RoseОценок пока нет
- Procedural SkillsДокумент26 страницProcedural Skillsmrcsexam.iranОценок пока нет
- Periop 101 Study Guide #1Документ18 страницPeriop 101 Study Guide #1Tawanda Boone-ShufordОценок пока нет
- CARDIAC SURGERY SSI PREVENTION CHECKLISTДокумент41 страницаCARDIAC SURGERY SSI PREVENTION CHECKLISTVenkata Raja sekhara Rao KetanaОценок пока нет
- Test Development HdowlingaДокумент13 страницTest Development Hdowlingaapi-178674977Оценок пока нет
- Revathi Papsmear ProcedureДокумент50 страницRevathi Papsmear ProcedureRevathi DadamОценок пока нет
- Dsa Cerebral AngiographyДокумент20 страницDsa Cerebral AngiographyLalaine De JesusОценок пока нет
- Before and After Radical Prostate Surgery: Information and Resource GuideОт EverandBefore and After Radical Prostate Surgery: Information and Resource GuideОценок пока нет
- Nucmed 7Документ33 страницыNucmed 7John Paul MarasiganОценок пока нет
- Barium Enema How The Test Will FeelДокумент19 страницBarium Enema How The Test Will Feeldonna-madongit-6792Оценок пока нет
- Macklon Covid Guidelines Webinar 25 May VersionДокумент37 страницMacklon Covid Guidelines Webinar 25 May VersionThuy Trang Nguyen ThiОценок пока нет
- Radiography and Mammography Procedures ExplainedДокумент28 страницRadiography and Mammography Procedures ExplainedAqee FarooqОценок пока нет
- Pap SmearДокумент32 страницыPap SmearAmira Nasir100% (1)
- Xrays 123Документ13 страницXrays 123Rasheed OladipupoОценок пока нет
- Guidance On Lung Function Testing: SARS COVID-19: Hse/HpscДокумент2 страницыGuidance On Lung Function Testing: SARS COVID-19: Hse/HpscEzequiel Tupac CarusoОценок пока нет
- ASWATHYДокумент61 страницаASWATHYJuvana LachuОценок пока нет
- COVID 19. 4 - 13 KashmerДокумент42 страницыCOVID 19. 4 - 13 KashmerIshfaq GanaiОценок пока нет
- COVID-19 Preparedness 14apr2020Документ13 страницCOVID-19 Preparedness 14apr2020Andre3893Оценок пока нет
- Diagnostic Imaging ProceduresДокумент6 страницDiagnostic Imaging ProceduresMichaela JapsayОценок пока нет
- Guide to Mediastinoscopy ProcedureДокумент10 страницGuide to Mediastinoscopy Procedureniña_ayonОценок пока нет
- Specialists in Reproductive Medicine & Surgery, P.A.: Definition: SchedulingДокумент3 страницыSpecialists in Reproductive Medicine & Surgery, P.A.: Definition: SchedulingjessicacookОценок пока нет
- Fluoroscopy - HysterosalpinogramДокумент5 страницFluoroscopy - HysterosalpinogramJosiah E. UmanaОценок пока нет
- Cervix Pre-Cancer Lession Tratment WorkshopДокумент64 страницыCervix Pre-Cancer Lession Tratment WorkshopsintiadamayantiОценок пока нет
- Nursong ResponsibilitiesДокумент4 страницыNursong ResponsibilitiesMichaela JapsayОценок пока нет
- Плаквенил - терапия - UCSF Adult COVID draft management guidelinesДокумент21 страницаПлаквенил - терапия - UCSF Adult COVID draft management guidelinesGuy MskОценок пока нет
- Hospital SopsДокумент12 страницHospital Sopspratimaz80% (5)
- Pre and Post Operative Care PrinciplesДокумент30 страницPre and Post Operative Care PrinciplesivanОценок пока нет
- COVID-19 Guidelines for MFM and OB-GYN PractitionersДокумент8 страницCOVID-19 Guidelines for MFM and OB-GYN PractitionersKismet LeeОценок пока нет
- Handout Breast CancerДокумент8 страницHandout Breast Cancernatalie pemberton-parrisОценок пока нет
- RAD044 Having An Ultrasound ScanДокумент5 страницRAD044 Having An Ultrasound ScanMuhammad Tariq AzizОценок пока нет
- Complete Blood Count PPT PresentationДокумент15 страницComplete Blood Count PPT PresentationShelley Ann Badayos0% (1)
- Consent Advice Laparoscopic Tubal OcclusionДокумент2 страницыConsent Advice Laparoscopic Tubal OcclusionKathJamesОценок пока нет
- Prostate CancerДокумент34 страницыProstate CancerKoRnflakes100% (1)
- A-Z of Neurosugery (April 2016 Update)Документ13 страницA-Z of Neurosugery (April 2016 Update)VamsiKrishnaChagalakondaОценок пока нет
- Cervical SmearДокумент16 страницCervical SmearĶHwola ƏľsHokryОценок пока нет
- 2008 High Risk Ob Us GuidelinesДокумент15 страниц2008 High Risk Ob Us GuidelinesCristina DruzianОценок пока нет
- Testicular Tumors The EndДокумент67 страницTesticular Tumors The EndRamesh ReddyОценок пока нет
- Nursing Skills Output (Nso) Week: 9 Arteriography: Ateneo de Zamboanga University College of NursingДокумент14 страницNursing Skills Output (Nso) Week: 9 Arteriography: Ateneo de Zamboanga University College of NursingMitzi BelamideОценок пока нет
- STANDARD PRACTICE GUIDELINES FOR DIAGNOSTIC RADIOLOGYДокумент40 страницSTANDARD PRACTICE GUIDELINES FOR DIAGNOSTIC RADIOLOGYRu RawОценок пока нет
- Radiotherapy For Rectal Cancer - A5 v2.0Документ24 страницыRadiotherapy For Rectal Cancer - A5 v2.0Diana MaicanОценок пока нет
- Principles of Gynecological Surgeries 1Документ127 страницPrinciples of Gynecological Surgeries 1Mohammad AlrefaiОценок пока нет
- Female SterilisationДокумент29 страницFemale SterilisationWilliams Emmanuel AdeyeyeОценок пока нет
- CRH Radiology Policies and ProceduresДокумент60 страницCRH Radiology Policies and ProceduresAbdul Saeed Shah100% (1)
- IOTA Simple Ultrasound Rules for Triage of Adnexal Mass: Experience from South IndiaДокумент49 страницIOTA Simple Ultrasound Rules for Triage of Adnexal Mass: Experience from South Indiashivangini sahayОценок пока нет
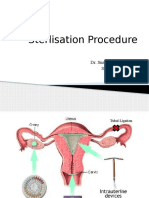
- Sterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalДокумент30 страницSterlisation Procedure: Dr. Sushruta Shrivastava SR Dept of OBGY AIIMS, BhopalsushrutaОценок пока нет
- PLACENTA PREVIA TOTALIS CaseДокумент19 страницPLACENTA PREVIA TOTALIS CasebobtagubaОценок пока нет
- Laparoscopy and Laparoscopic SurgeryДокумент4 страницыLaparoscopy and Laparoscopic SurgerySidra AnjumОценок пока нет
- Data Peserta Level IДокумент20 страницData Peserta Level Ifariska amanizataОценок пока нет
- Formulir Pendaftaran Munaqasyah Level 2 (Jawaban)Документ4 страницыFormulir Pendaftaran Munaqasyah Level 2 (Jawaban)fariska amanizataОценок пока нет
- Force EnrichmentДокумент2 страницыForce Enrichmentfariska amanizataОценок пока нет
- Mathematics Enrichment Chapter 12'Документ2 страницыMathematics Enrichment Chapter 12'fariska amanizataОценок пока нет
- 28.normal and Abnormal LaborДокумент19 страниц28.normal and Abnormal Laborfariska amanizataОценок пока нет
- 3RD Grade Unit 7 & 8Документ4 страницы3RD Grade Unit 7 & 8fariska amanizataОценок пока нет
- Tanya Apa Saja: Menopouse DiniДокумент1 страницаTanya Apa Saja: Menopouse Dinifariska amanizataОценок пока нет
- Lecture 4 FGRДокумент32 страницыLecture 4 FGRfariska amanizataОценок пока нет
- Fetal skull diameters and presentationsДокумент5 страницFetal skull diameters and presentationsfariska amanizataОценок пока нет
- Grade 3 Food ProductionДокумент2 страницыGrade 3 Food Productionfariska amanizataОценок пока нет
- Buy 1 Get 1 ATASANДокумент12 страницBuy 1 Get 1 ATASANfariska amanizataОценок пока нет
- Enrichment Math Chapter 14Документ2 страницыEnrichment Math Chapter 14fariska amanizataОценок пока нет
- ENRICHMENT OF SCIENCE - Sense 2Документ2 страницыENRICHMENT OF SCIENCE - Sense 2fariska amanizataОценок пока нет
- Grade 3 Chapter 4.1 Parts of Flowering Plant WorksheetДокумент2 страницыGrade 3 Chapter 4.1 Parts of Flowering Plant Worksheetfariska amanizataОценок пока нет
- Enrichment MultiplicationДокумент1 страницаEnrichment Multiplicationfariska amanizataОценок пока нет
- Grade 3 Chapter 4.1 Parts of Flowering Plant WorksheetДокумент2 страницыGrade 3 Chapter 4.1 Parts of Flowering Plant Worksheetfariska amanizataОценок пока нет
- Enrichment Mathematics Chapter 8Документ2 страницыEnrichment Mathematics Chapter 8fariska amanizataОценок пока нет
- Enrichment Math Chapter 5Документ2 страницыEnrichment Math Chapter 5fariska amanizataОценок пока нет
- Lesson Worksheet: Taking Care of Teeth: ScienceДокумент3 страницыLesson Worksheet: Taking Care of Teeth: Sciencefariska amanizataОценок пока нет
- 3RD Grade Unit 7 & 8Документ4 страницы3RD Grade Unit 7 & 8fariska amanizataОценок пока нет
- Webinar Helicobacter Pylori 080720 - Invitation PDFДокумент1 страницаWebinar Helicobacter Pylori 080720 - Invitation PDFfariska amanizataОценок пока нет
- Pravastatin Suppresses Inflammatory Cytokines and Endothelial Activation in Patients at Risk of Developing Preeclampsia INOVASIA Study-1Документ9 страницPravastatin Suppresses Inflammatory Cytokines and Endothelial Activation in Patients at Risk of Developing Preeclampsia INOVASIA Study-1fariska amanizataОценок пока нет
- CDC: Understanding The Difference Between MasksДокумент1 страницаCDC: Understanding The Difference Between MasksEd PraetorianОценок пока нет
- SARS-CoV-2 Detected in Placental SamplesДокумент7 страницSARS-CoV-2 Detected in Placental Samplesfariska amanizataОценок пока нет
- Patient-Centered Care for Pregnant Patients during COVID-19Документ1 страницаPatient-Centered Care for Pregnant Patients during COVID-19fariska amanizataОценок пока нет
- Materi Science Natural PhenomenaДокумент2 страницыMateri Science Natural Phenomenafariska amanizataОценок пока нет
- MATHEMATICS PRACTICE 7-8 FixДокумент1 страницаMATHEMATICS PRACTICE 7-8 Fixfariska amanizataОценок пока нет
- Materi Science Natural PhenomenaДокумент2 страницыMateri Science Natural Phenomenafariska amanizataОценок пока нет
- CDC: Understanding The Difference Between MasksДокумент1 страницаCDC: Understanding The Difference Between MasksEd PraetorianОценок пока нет
- Ofper 1 Application For Seagoing AppointmentДокумент4 страницыOfper 1 Application For Seagoing AppointmentNarayana ReddyОценок пока нет
- !!!Логос - конференц10.12.21 копіяДокумент141 страница!!!Логос - конференц10.12.21 копіяНаталія БондарОценок пока нет
- Simba s7d Long Hole Drill RigДокумент2 страницыSimba s7d Long Hole Drill RigJaime Asis LopezОценок пока нет
- The Smith Generator BlueprintsДокумент36 страницThe Smith Generator BlueprintsZoran AleksicОценок пока нет
- Extrajudicial Settlement of Estate Rule 74, Section 1 ChecklistДокумент8 страницExtrajudicial Settlement of Estate Rule 74, Section 1 ChecklistMsyang Ann Corbo DiazОценок пока нет
- Srimanta Sankaradeva Universityof Health SciencesДокумент3 страницыSrimanta Sankaradeva Universityof Health SciencesTemple RunОценок пока нет
- CBSE Class 6 Whole Numbers WorksheetДокумент2 страницыCBSE Class 6 Whole Numbers WorksheetPriyaprasad PandaОценок пока нет
- Computer Networks Transmission Media: Dr. Mohammad AdlyДокумент14 страницComputer Networks Transmission Media: Dr. Mohammad AdlyRichthofen Flies Bf109Оценок пока нет
- NLP Business Practitioner Certification Course OutlineДокумент11 страницNLP Business Practitioner Certification Course OutlineabobeedoОценок пока нет
- Why Choose Medicine As A CareerДокумент25 страницWhy Choose Medicine As A CareerVinod KumarОценок пока нет
- Mobile ApplicationДокумент2 страницыMobile Applicationdarebusi1Оценок пока нет
- NABARD road inspection report formatДокумент24 страницыNABARD road inspection report formatSrinivas PОценок пока нет
- IELTS Speaking Q&AДокумент17 страницIELTS Speaking Q&ABDApp Star100% (1)
- Money Laundering in Online Trading RegulationДокумент8 страницMoney Laundering in Online Trading RegulationSiti Rabiah MagfirohОценок пока нет
- Guide To Raising Capital From Angel Investors Ebook From The Startup Garage PDFДокумент20 страницGuide To Raising Capital From Angel Investors Ebook From The Startup Garage PDFLars VonTurboОценок пока нет
- Duca Industries March 2023 pay slip for Dipankar MondalДокумент1 страницаDuca Industries March 2023 pay slip for Dipankar MondalPritam GoswamiОценок пока нет
- U2 All That You Can't Leave BehindДокумент82 страницыU2 All That You Can't Leave BehindFranck UrsiniОценок пока нет
- Ball Valves Pentair Valves and ControlsДокумент16 страницBall Valves Pentair Valves and ControlsABDUL KADHARОценок пока нет
- Shopping Mall: Computer Application - IiiДокумент15 страницShopping Mall: Computer Application - IiiShadowdare VirkОценок пока нет
- GS16 Gas Valve: With On-Board DriverДокумент4 страницыGS16 Gas Valve: With On-Board DriverProcurement PardisanОценок пока нет
- Special Power of Attorney: Benedict Joseph M. CruzДокумент1 страницаSpecial Power of Attorney: Benedict Joseph M. CruzJson GalvezОценок пока нет
- SBI Sample PaperДокумент283 страницыSBI Sample Paperbeintouch1430% (1)
- Crystallizers: Chapter 16 Cost Accounting and Capital Cost EstimationДокумент1 страницаCrystallizers: Chapter 16 Cost Accounting and Capital Cost EstimationDeiver Enrique SampayoОценок пока нет
- PEDs and InterferenceДокумент28 страницPEDs and Interferencezakool21Оценок пока нет
- Gabinete STS Activity1Документ2 страницыGabinete STS Activity1Anthony GabineteОценок пока нет
- SolBridge Application 2012Документ14 страницSolBridge Application 2012Corissa WandmacherОценок пока нет
- Exercise-01: JEE-PhysicsДокумент52 страницыExercise-01: JEE-Physicsjk rОценок пока нет
- EIRA v0.8.1 Beta OverviewДокумент33 страницыEIRA v0.8.1 Beta OverviewAlexQuiñonesNietoОценок пока нет
- France Winckler Final Rev 1Документ14 страницFrance Winckler Final Rev 1Luciano Junior100% (1)
- Photosynthesis Lab ReportДокумент7 страницPhotosynthesis Lab ReportTishaОценок пока нет