Вам также может понравиться
- Anatomy of The Female Reproductive SystemДокумент62 страницыAnatomy of The Female Reproductive SystemBibek GajmerОценок пока нет
- Perineum 180922120553 PDFДокумент45 страницPerineum 180922120553 PDFFazle RabbiОценок пока нет
- Ma. Elizabeth F. FontanillaДокумент48 страницMa. Elizabeth F. Fontanillatam mei100% (1)
- Bladder&UrethraДокумент36 страницBladder&UrethraBalaji KarunakaranОценок пока нет
- Abdomen (Repaired)Документ174 страницыAbdomen (Repaired)Merellyn Hurtado PachecoОценок пока нет
- Abdominal Wall: Muh. Iqbal Basri Anatomy Department Hasanuddin UniversityДокумент33 страницыAbdominal Wall: Muh. Iqbal Basri Anatomy Department Hasanuddin UniversityDavid ChristianОценок пока нет
- Abdomen (Repaired)Документ172 страницыAbdomen (Repaired)OstazОценок пока нет
- Key PointsДокумент34 страницыKey PointsSe YunОценок пока нет
- Dinding Abdomen PSIKДокумент79 страницDinding Abdomen PSIKSondang DamanikОценок пока нет
- Ureters Urinary Bladder UrethraДокумент20 страницUreters Urinary Bladder UrethraFlora PopaОценок пока нет
- Abdominal Wall and PeritoneumДокумент25 страницAbdominal Wall and PeritoneumZeyneb BoutouchentОценок пока нет
- 13-The Anal TriangleДокумент36 страниц13-The Anal TriangleoyomziicОценок пока нет
- Anatomy of Inguinal CanalДокумент10 страницAnatomy of Inguinal CanalsaisoniaОценок пока нет
- EMRCS Abdomin AnatomyДокумент54 страницыEMRCS Abdomin AnatomyShakirОценок пока нет
- UntitledДокумент7 страницUntitledDania Ibraheem100% (1)
- Lec 6Документ7 страницLec 6Dania IbraheemОценок пока нет
- Anatomy, Lecture 9, Abdominal WallДокумент22 страницыAnatomy, Lecture 9, Abdominal WallAli Al-QudsiОценок пока нет
- PERINEUMДокумент24 страницыPERINEUMmhr27112002Оценок пока нет
- Rectum and Anal CanalДокумент44 страницыRectum and Anal CanalAayush BhattaОценок пока нет
- APOSTLE JOHN'S ABDOMEN NOTE - WPS OfficeДокумент19 страницAPOSTLE JOHN'S ABDOMEN NOTE - WPS OfficeOROKE JOHN EJEОценок пока нет
- 01 Anatomy of Female Genital SystemДокумент63 страницы01 Anatomy of Female Genital Systemtania100% (2)
- Abdominal Wall and HerniaДокумент35 страницAbdominal Wall and HerniaMohammad BanisalmanОценок пока нет
- Gastrointestinal SystemДокумент56 страницGastrointestinal SystemPaula Daniela Quimbayo AcuñaОценок пока нет
- Abdominal HerniasДокумент38 страницAbdominal HerniasHafizah HoshniОценок пока нет
- Gynecology - Anatomy: Dr. Fidia MumtahanaДокумент125 страницGynecology - Anatomy: Dr. Fidia MumtahanaSonny JhaОценок пока нет
- Anatomy of The Anterior Abdominal Wall Part II: Lecture - 2Документ34 страницыAnatomy of The Anterior Abdominal Wall Part II: Lecture - 2Ahmed OudahОценок пока нет
- Anatomy of GIT For PCII Students..Документ106 страницAnatomy of GIT For PCII Students..AMANUEL HABTEWOLDОценок пока нет
- GRDA Male Pelvis Female PelvisДокумент20 страницGRDA Male Pelvis Female PelvisKingОценок пока нет
- Anatomy of Fallopian Tube & OvaryДокумент89 страницAnatomy of Fallopian Tube & OvaryAsma AijazОценок пока нет
- Female Reproductive SystemДокумент46 страницFemale Reproductive SystemAzza100% (11)
- Abdominal Wall Learning ObjectivesДокумент7 страницAbdominal Wall Learning ObjectivesMadison KommorОценок пока нет
- Physio OB Maternal Anatomy External and Internal Generative Organs PPT 2Документ67 страницPhysio OB Maternal Anatomy External and Internal Generative Organs PPT 2Janine SergioОценок пока нет
- Inguinal CanalДокумент48 страницInguinal CanalMahi100% (1)
- The PerineumДокумент3 страницыThe PerineumSanjay KishoreОценок пока нет
- Anatomy Materials AbdomenДокумент21 страницаAnatomy Materials AbdomenEmilee TuОценок пока нет
- Penis & DisordersДокумент54 страницыPenis & Disordersshivay100% (1)
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreДокумент36 страницOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorОценок пока нет
- Inguinal Canal: DR - Lubna NazliДокумент28 страницInguinal Canal: DR - Lubna NazliAhmed AminОценок пока нет
- Inguinal Canal: Medial One-Half of The Inguinal Ligament Also Known As Poupart LigamentДокумент4 страницыInguinal Canal: Medial One-Half of The Inguinal Ligament Also Known As Poupart LigamentDivya RanasariaОценок пока нет
- Maternal Anatomy WilliamsДокумент52 страницыMaternal Anatomy WilliamsMariane Tejano100% (1)
- Female Reproductive SystemДокумент40 страницFemale Reproductive SystemSAYMABANUОценок пока нет
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreДокумент36 страницOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreYoAmoNYCОценок пока нет
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreДокумент36 страницOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorОценок пока нет
- A No RectalДокумент34 страницыA No RectalSyarafina AzmanОценок пока нет
- Anterior Abdominal WallДокумент39 страницAnterior Abdominal WallZllison Mae Teodoro MangabatОценок пока нет
- Abdominal WallДокумент75 страницAbdominal WallJojo RyelciusОценок пока нет
- Anatomy of The Female ReproductionДокумент108 страницAnatomy of The Female ReproductionDaisy HamdaliОценок пока нет
- Female Reproductive System-AnatomyДокумент57 страницFemale Reproductive System-AnatomyEstellaОценок пока нет
- Anterior Abdominal WallДокумент47 страницAnterior Abdominal WallJohn NgumbiОценок пока нет
- Groin AnatomyДокумент7 страницGroin AnatomyLorenzo Daniel AntonioОценок пока нет
- HerniaДокумент106 страницHerniaDr-Mohammad Ali-Fayiz Al TamimiОценок пока нет
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreДокумент28 страницOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorОценок пока нет
- Anatomy Abdominal WallДокумент87 страницAnatomy Abdominal WallMRS DR NIDHI SHARMA VISHWAKARMA100% (2)
- Anatomy of Female Reproductive Organs: Dr.M.Mahalakshmi Assistant Professor Government Chengalpattu Medical CollegeДокумент20 страницAnatomy of Female Reproductive Organs: Dr.M.Mahalakshmi Assistant Professor Government Chengalpattu Medical Collegepranu6789Оценок пока нет
- ANATOMY: Pelvic 5Документ23 страницыANATOMY: Pelvic 5Nur Liyana MohamadОценок пока нет
- RectumДокумент43 страницыRectummidhunramesh007100% (4)
- Surgical Anatomy-Anal Canal: Dr. Belal MansoorДокумент79 страницSurgical Anatomy-Anal Canal: Dr. Belal MansoorYogi drОценок пока нет
- Full Notes Embryo DetailedДокумент33 страницыFull Notes Embryo DetailedJoseph KimОценок пока нет
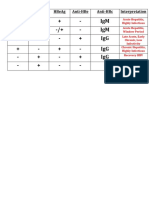
- HBV Antibody InterpretationДокумент1 страницаHBV Antibody InterpretationJoseph KimОценок пока нет
- Physiology DES: Biruk A. (Balemaye@sgu - Edu) & Sami Ahmed. (Sahmed10@sgu - Edu)Документ56 страницPhysiology DES: Biruk A. (Balemaye@sgu - Edu) & Sami Ahmed. (Sahmed10@sgu - Edu)Joseph KimОценок пока нет
- First Aid Virology SectionДокумент15 страницFirst Aid Virology SectionJoseph KimОценок пока нет
- Physio-DES-6 (Cardiac)Документ56 страницPhysio-DES-6 (Cardiac)Joseph Kim100% (1)
- CH 18 Cholesterol Metabolism: Biochem Block 3 NotesДокумент38 страницCH 18 Cholesterol Metabolism: Biochem Block 3 NotesJoseph KimОценок пока нет
- Nbme 12 Section 1 AnswersДокумент4 страницыNbme 12 Section 1 AnswersDavid LeeОценок пока нет
- Clinical Integration: Lymphatic & Respiratory SystemsДокумент13 страницClinical Integration: Lymphatic & Respiratory SystemsJoseph KimОценок пока нет
- Grand Anse To True Blue Weekend Bus 2 Spring 2020Документ1 страницаGrand Anse To True Blue Weekend Bus 2 Spring 2020Joseph KimОценок пока нет
- A True Blue To Grand Anse Master Weekday Spring 2020Документ1 страницаA True Blue To Grand Anse Master Weekday Spring 2020Joseph KimОценок пока нет
- Respiratory System: Lab Interactive SessionДокумент20 страницRespiratory System: Lab Interactive SessionJoseph KimОценок пока нет
- Lymphatic System: Lab Interactive SessionДокумент24 страницыLymphatic System: Lab Interactive SessionJoseph KimОценок пока нет
- DiGeorge Case Fall 2016Документ3 страницыDiGeorge Case Fall 2016Joseph KimОценок пока нет
- DiGeorge Case Fall 2016 PDFДокумент2 страницыDiGeorge Case Fall 2016 PDFJoseph KimОценок пока нет
- Virus ClassificationДокумент1 страницаVirus ClassificationJoseph KimОценок пока нет
- E True Blue To True Blue Inn Spring 2020Документ2 страницыE True Blue To True Blue Inn Spring 2020Joseph KimОценок пока нет
- DiGeorge Case Fall 2016 PDFДокумент2 страницыDiGeorge Case Fall 2016 PDFJoseph KimОценок пока нет
- First Aid Virology SectionДокумент15 страницFirst Aid Virology SectionJoseph KimОценок пока нет
- 02 A Table of Molec Diagnostic Techniques - SP 2016Документ4 страницы02 A Table of Molec Diagnostic Techniques - SP 2016Joseph KimОценок пока нет
- RNA Viruses ChartДокумент1 страницаRNA Viruses ChartJoseph KimОценок пока нет
- VirusesДокумент19 страницVirusesJoseph KimОценок пока нет
- CPR MCQДокумент18 страницCPR MCQJoseph KimОценок пока нет
- CPR ImcqДокумент9 страницCPR ImcqJoseph KimОценок пока нет
- CPR MCQДокумент11 страницCPR MCQJoseph KimОценок пока нет
- FoodGroupsAndCaloriesReport DetailedДокумент7 страницFoodGroupsAndCaloriesReport DetailedJoseph KimОценок пока нет
- Physio Lab CasesДокумент4 страницыPhysio Lab CasesJoseph KimОценок пока нет
- Biochemistry DES 9Документ47 страницBiochemistry DES 9Joseph KimОценок пока нет
- Applications of MathematicsДокумент35 страницApplications of MathematicsRamdas Sonawane100% (1)
- Chapter 123 RevisedДокумент23 страницыChapter 123 RevisedCristy Ann BallanОценок пока нет
- MML3 Journal To CapcomДокумент103 страницыMML3 Journal To CapcomFer BarcenaОценок пока нет
- Gathering Package 2023Документ2 страницыGathering Package 2023Sudiantara abasОценок пока нет
- Salva v. MakalintalДокумент2 страницыSalva v. MakalintalGain DeeОценок пока нет
- Spine Beam - SCHEME 4Документ28 страницSpine Beam - SCHEME 4Edi ObrayanОценок пока нет
- CE5215-Theory and Applications of Cement CompositesДокумент10 страницCE5215-Theory and Applications of Cement CompositesSivaramakrishnaNalluriОценок пока нет
- Civil NatureДокумент3 страницыCivil NatureZ_Jahangeer100% (4)
- Irrig in AfricaДокумент64 страницыIrrig in Africaer viОценок пока нет
- Black BookДокумент28 страницBlack Bookshubham50% (2)
- Woodward GCP30 Configuration 37278 - BДокумент174 страницыWoodward GCP30 Configuration 37278 - BDave Potter100% (1)
- h6811 Datadomain DsДокумент5 страницh6811 Datadomain DsChristian EstebanОценок пока нет
- Admission Notice: Weekend Masters Program (WMES)Документ4 страницыAdmission Notice: Weekend Masters Program (WMES)masud100% (1)
- Revenue Management Session 1: Introduction To Pricing OptimizationДокумент55 страницRevenue Management Session 1: Introduction To Pricing OptimizationDuc NguyenОценок пока нет
- Chapter 1 Hospital and Clinical Pharmacy Choplete PDF Notes D.Pharma 2nd Notes PDF NoteskartsДокумент7 страницChapter 1 Hospital and Clinical Pharmacy Choplete PDF Notes D.Pharma 2nd Notes PDF NoteskartsDrx Brajendra LodhiОценок пока нет
- Enumerator ResumeДокумент1 страницаEnumerator Resumesaid mohamudОценок пока нет
- Org ChartДокумент1 страницаOrg Chart2021-101781Оценок пока нет
- Computerized AccountingДокумент14 страницComputerized Accountinglayyah2013Оценок пока нет
- Indirect Teaching Strategy??: Name: Topic: Under SupervisionДокумент9 страницIndirect Teaching Strategy??: Name: Topic: Under SupervisionSeham FouadОценок пока нет
- SKF LGMT-2 Data SheetДокумент2 страницыSKF LGMT-2 Data SheetRahul SharmaОценок пока нет
- Drug Study TemplateДокумент2 страницыDrug Study TemplateKistlerzane CABALLEROОценок пока нет
- Mentorship ICT at A GlanceДокумент5 страницMentorship ICT at A GlanceTeachers Without Borders0% (1)
- Safety Inspection Checklist Project: Location: Inspector: DateДокумент2 страницыSafety Inspection Checklist Project: Location: Inspector: Dateyono DaryonoОценок пока нет
- CC Anbcc FD 002 Enr0Документ5 страницCC Anbcc FD 002 Enr0ssierroОценок пока нет
- Nguyen Dang Bao Tran - s3801633 - Assignment 1 Business Report - BAFI3184 Business FinanceДокумент14 страницNguyen Dang Bao Tran - s3801633 - Assignment 1 Business Report - BAFI3184 Business FinanceNgọc MaiОценок пока нет
- ILRF Soccer Ball ReportДокумент40 страницILRF Soccer Ball ReportgabalauiОценок пока нет
- Rules On Evidence PDFДокумент35 страницRules On Evidence PDFEuodia HodeshОценок пока нет
- Expected MCQs CompressedДокумент31 страницаExpected MCQs CompressedAdithya kesavОценок пока нет
- Idmt Curve CalulationДокумент5 страницIdmt Curve CalulationHimesh NairОценок пока нет
- Strategic Management ModelsДокумент4 страницыStrategic Management ModelsBarno NicholusОценок пока нет
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (24)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (169)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (3)
- Gut: the new and revised Sunday Times bestsellerОт EverandGut: the new and revised Sunday Times bestsellerРейтинг: 4 из 5 звезд4/5 (392)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (253)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningОт EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningРейтинг: 4 из 5 звезд4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceОт EverandTo Explain the World: The Discovery of Modern ScienceРейтинг: 3.5 из 5 звезд3.5/5 (51)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (44)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisОт EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (9)