Вам также может понравиться
- 00 Winch Inspection Check ListДокумент1 страница00 Winch Inspection Check ListGyanendra Narayan Nayak90% (10)
- JAPL-F-HE-001-Weekly Grader Inspection ChecklistДокумент2 страницыJAPL-F-HE-001-Weekly Grader Inspection ChecklistAli HassanОценок пока нет
- Short Employee Service AssessmentДокумент2 страницыShort Employee Service Assessmentdennisjuntak100% (1)
- Safety Data Sheet: 1. Product and Company IdentificationДокумент20 страницSafety Data Sheet: 1. Product and Company IdentificationPubcrawlОценок пока нет
- SPI HSE FR 01 Foundation ChecklistДокумент1 страницаSPI HSE FR 01 Foundation ChecklistChandan KumarОценок пока нет
- VE ST HE LM ET SH OE S GO GG LES: Violation DateДокумент1 страницаVE ST HE LM ET SH OE S GO GG LES: Violation DateSubzone ThreeОценок пока нет
- HSE Weekly Inspection CLOSEOUT - R No. 01 Al SowaidiДокумент7 страницHSE Weekly Inspection CLOSEOUT - R No. 01 Al SowaidiAkhilesh ArunachalamОценок пока нет
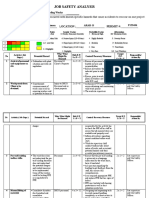
- Water Proofing JSAДокумент9 страницWater Proofing JSARamОценок пока нет
- Weekly Safety Management Walkthrough Report: Gas Compression Project DepartmentДокумент6 страницWeekly Safety Management Walkthrough Report: Gas Compression Project DepartmentMuhammad TariqОценок пока нет
- Plant & System ObservationДокумент4 страницыPlant & System ObservationZeeshan Pathan0% (1)
- Acf-Mra-064 - SCДокумент1 страницаAcf-Mra-064 - SCFateh AliyaОценок пока нет
- Mom For Table To Drill MeetingДокумент2 страницыMom For Table To Drill MeetingChaudhary Wasim MurtazaОценок пока нет
- Contractor Environmental Monthly Returns: Monthly Air Quality Sampling Data AttachedДокумент3 страницыContractor Environmental Monthly Returns: Monthly Air Quality Sampling Data AttachedJayvee Baradas ValdezОценок пока нет
- C - 6 Crane & Lifting Equipment StandartДокумент4 страницыC - 6 Crane & Lifting Equipment StandartwawanОценок пока нет
- Deficiencies of All TCF ReportsДокумент4 страницыDeficiencies of All TCF ReportsMuhammad TariqОценок пока нет
- HIP-Wastewater Revision 03Документ14 страницHIP-Wastewater Revision 03Darius DsouzaОценок пока нет
- 3.3.4 Monthly Suction Septic Tank LogДокумент2 страницы3.3.4 Monthly Suction Septic Tank LogSubzone ThreeОценок пока нет
- Weekly Report As of September 12Документ45 страницWeekly Report As of September 12Cesar DuriasОценок пока нет
- Lifting Calculation Per LocationДокумент1 страницаLifting Calculation Per LocationSubzone ThreeОценок пока нет
- Weekly Safety Management Walkthrough Report: Gas Compression Project DepartmentДокумент12 страницWeekly Safety Management Walkthrough Report: Gas Compression Project DepartmentSheri DiĺlОценок пока нет
- BVI-HSE Daily Report 20220816Документ3 страницыBVI-HSE Daily Report 20220816Muhammad IrfanОценок пока нет
- Night Work Inspection ChecklistДокумент1 страницаNight Work Inspection ChecklistAdarsh sОценок пока нет
- IMS-39 Job Specific Training RecordДокумент1 страницаIMS-39 Job Specific Training RecordRísês ÃfrözОценок пока нет
- HSE Weekly Review MOM 11.01.2023Документ2 страницыHSE Weekly Review MOM 11.01.2023APEX STRUCTUREОценок пока нет
- Equipment Check List Report (Monthly) Asphalt Cutter::::::: ConditionДокумент2 страницыEquipment Check List Report (Monthly) Asphalt Cutter::::::: ConditionAbdus SamadОценок пока нет
- Emergency Drill ReportДокумент10 страницEmergency Drill ReportSheri DiĺlОценок пока нет
- Reynaldo Darcera: Project Management Contractor Near-Miss at Worksite ReportДокумент15 страницReynaldo Darcera: Project Management Contractor Near-Miss at Worksite ReportAyaz AhmadОценок пока нет
- HIP-Rabigh Development ProjectДокумент5 страницHIP-Rabigh Development ProjectDarius DsouzaОценок пока нет
- Safety Meeting PHTДокумент2 страницыSafety Meeting PHTMohamad Hidayat Zainul Masri100% (2)
- Hse Car 2Документ3 страницыHse Car 2Mohd Fadli100% (1)
- Monsoon Safety AdvisoryДокумент16 страницMonsoon Safety AdvisoryRajneesh KumarОценок пока нет
- F-49 Full Body Harness Inspection ChecklistДокумент1 страницаF-49 Full Body Harness Inspection ChecklistSKH Culture100% (1)
- Housekeeping CampaignДокумент5 страницHousekeeping CampaignAhmad SaeedОценок пока нет
- 2 Heat Stess DRILL (9 June 2020)Документ14 страниц2 Heat Stess DRILL (9 June 2020)Usman RajputОценок пока нет
- Pakaian Kerja Safety Katalog Nasional 2017Документ3 страницыPakaian Kerja Safety Katalog Nasional 2017deweparumamenОценок пока нет
- Acf-Mra-063 - UaДокумент1 страницаAcf-Mra-063 - UaFateh AliyaОценок пока нет
- Nearmiss Trending AnalysisДокумент40 страницNearmiss Trending AnalysisTayyab MayoОценок пока нет
- Compressed Gas CylinderДокумент4 страницыCompressed Gas CylinderjeyesbelmenОценок пока нет
- Survey Work HSE Risk AssessmentsДокумент2 страницыSurvey Work HSE Risk AssessmentsSarfraz RandhawaОценок пока нет
- Action Plan (Al-Gihaz Gregar Ohtl)Документ2 страницыAction Plan (Al-Gihaz Gregar Ohtl)Ahsan MumtazОценок пока нет
- Ev05 - Safety Task Analysis Reduction - Star Card in Different LanguageДокумент3 страницыEv05 - Safety Task Analysis Reduction - Star Card in Different LanguageFrancis Enriquez TanОценок пока нет
- Sor-Landscape-Ppe5 29 Dec. 2020Документ1 страницаSor-Landscape-Ppe5 29 Dec. 2020haniОценок пока нет
- 129th HSJV Weekly MeetingДокумент29 страниц129th HSJV Weekly MeetingHumpy DumpyОценок пока нет
- MIP17 Close Out ReportДокумент9 страницMIP17 Close Out ReportAmeerHamzaWarraich100% (1)
- Appendix-AC, Guide For Working at HeightsДокумент23 страницыAppendix-AC, Guide For Working at HeightsApm FoumilОценок пока нет
- HSEДокумент2 страницыHSEPanchdev KumarОценок пока нет
- 07-2011 Concrete PumpДокумент2 страницы07-2011 Concrete PumpBlake Charles Diniz MarquesОценок пока нет
- Obtain Authorisation Before Overriding or Disabling Safety ControlsДокумент9 страницObtain Authorisation Before Overriding or Disabling Safety ControlsKathleen Faith C. BrionesОценок пока нет
- Construction Site Inspection Check List ALMCДокумент2 страницыConstruction Site Inspection Check List ALMCAmeerHamzaWarraichОценок пока нет
- Annexure B Safety Campaign PlanДокумент1 страницаAnnexure B Safety Campaign PlanSandeep KumarОценок пока нет
- F.hse.07 Work PermitДокумент4 страницыF.hse.07 Work PermitMOJIBОценок пока нет
- BVI-HSE Daily Report 20220818Документ3 страницыBVI-HSE Daily Report 20220818Muhammad IrfanОценок пока нет
- Disciplinary Action ReportДокумент1 страницаDisciplinary Action Reportshayne rosanes100% (1)
- Excavation and Shoring ChecklistДокумент1 страницаExcavation and Shoring ChecklistFrancis Enriquez TanОценок пока нет
- Work Permit-Form PDFДокумент1 страницаWork Permit-Form PDFNijo JosephОценок пока нет
- Drp001-Ouf-Inc-Gmd-Z-000-041-S1. C4Документ26 страницDrp001-Ouf-Inc-Gmd-Z-000-041-S1. C4rodman823Оценок пока нет
- Project Weekly Hse Report: 50Mw Indus Wind Energy LimitedДокумент6 страницProject Weekly Hse Report: 50Mw Indus Wind Energy LimitedRaza Muhammad Soomro100% (1)
- Near Miss Incident Report OCLДокумент3 страницыNear Miss Incident Report OCLThusithaОценок пока нет
- Water Tank ChecklistДокумент1 страницаWater Tank ChecklistIndermohan MehtaОценок пока нет
- Eye Wash Weekly ChecklistДокумент1 страницаEye Wash Weekly ChecklistSreejith SureshОценок пока нет
- Covid-19 Daily Screening Form at Site Entry GateДокумент1 страницаCovid-19 Daily Screening Form at Site Entry GateGyanendra Narayan NayakОценок пока нет
- Dial Phase 3A Project Risk Index For Hira: ActivityДокумент2 страницыDial Phase 3A Project Risk Index For Hira: ActivityGyanendra Narayan NayakОценок пока нет
- HIRA - COVID 19 Prevention and ControlsДокумент17 страницHIRA - COVID 19 Prevention and ControlsGyanendra Narayan NayakОценок пока нет
- Elcb Checking Format-TДокумент1 страницаElcb Checking Format-TGyanendra Narayan NayakОценок пока нет
- Caution Compressed Gas PDFДокумент1 страницаCaution Compressed Gas PDFGyanendra Narayan NayakОценок пока нет
- BHEL Gas Cutting Set Inspection Formate - Daily.Документ1 страницаBHEL Gas Cutting Set Inspection Formate - Daily.Gyanendra Narayan NayakОценок пока нет
- Electrical Safety Inspection Checklist-FДокумент2 страницыElectrical Safety Inspection Checklist-FGyanendra Narayan Nayak89% (9)
- BHEL Crane & Hydra Check ListДокумент1 страницаBHEL Crane & Hydra Check ListGyanendra Narayan NayakОценок пока нет
- BHEL Earth Pit Test ReportДокумент2 страницыBHEL Earth Pit Test ReportGyanendra Narayan NayakОценок пока нет
- BHEL Welding Machine Check ListДокумент1 страницаBHEL Welding Machine Check ListGyanendra Narayan NayakОценок пока нет
- BHEL Fire Extinguishers Inspection ChecklistДокумент1 страницаBHEL Fire Extinguishers Inspection ChecklistGyanendra Narayan NayakОценок пока нет
- BHEL Full Body HarnessДокумент3 страницыBHEL Full Body HarnessGyanendra Narayan NayakОценок пока нет
- Awadh Kulkarni - IS 14489Документ23 страницыAwadh Kulkarni - IS 14489Gyanendra Narayan NayakОценок пока нет
- NSCI Internal Occupational Safety & Health (OSH) Auditor's Course Reading Material 05-07 October 2020Документ256 страницNSCI Internal Occupational Safety & Health (OSH) Auditor's Course Reading Material 05-07 October 2020Gyanendra Narayan NayakОценок пока нет
- Ecat Fire Extinguisher AFFF Foam Data SheetДокумент1 страницаEcat Fire Extinguisher AFFF Foam Data SheetGyanendra Narayan NayakОценок пока нет
- Weld Manual 4 PowerДокумент77 страницWeld Manual 4 PowerGyanendra Narayan NayakОценок пока нет
- Hazard Identification and Risk Assessment VirtualДокумент33 страницыHazard Identification and Risk Assessment VirtualGyanendra Narayan Nayak100% (1)
- Documentation CheckingДокумент13 страницDocumentation CheckingGyanendra Narayan Nayak100% (1)
- OSH Management - Training - 27 - 7 - 2020Документ27 страницOSH Management - Training - 27 - 7 - 2020Gyanendra Narayan NayakОценок пока нет
- Techniques of Collecting InformationДокумент10 страницTechniques of Collecting InformationGyanendra Narayan NayakОценок пока нет
- Techniques of Report Writing VirtualДокумент10 страницTechniques of Report Writing VirtualGyanendra Narayan NayakОценок пока нет
- Above Ground TanksДокумент6 страницAbove Ground TanksGyanendra Narayan NayakОценок пока нет
- National Safety Council, India: Overview of Indian Standard and Statutes Related To Occupational Health & Safety AuditДокумент26 страницNational Safety Council, India: Overview of Indian Standard and Statutes Related To Occupational Health & Safety AuditGyanendra Narayan NayakОценок пока нет
- A-7 Emergency PreparednessДокумент12 страницA-7 Emergency PreparednessGyanendra Narayan NayakОценок пока нет
- A-4 Fire and Explosion HazardsДокумент21 страницаA-4 Fire and Explosion HazardsGyanendra Narayan NayakОценок пока нет