Вам также может понравиться
- Differentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)От EverandDifferentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)Оценок пока нет
- MorphineДокумент4 страницыMorphineMARITIM GEOFFREY KIPLANGATОценок пока нет
- Local Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)От EverandLocal Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)Оценок пока нет
- 4 SeizuresДокумент11 страниц4 SeizuresApple MaeОценок пока нет
- My Mifespristone and Misoprostol Story: How I used mifepristone and misoprostol for a successful medical abortion and all you must know about these abortion pillsОт EverandMy Mifespristone and Misoprostol Story: How I used mifepristone and misoprostol for a successful medical abortion and all you must know about these abortion pillsОценок пока нет
- Drug Study: Pharmacokinetics Absorption SiteДокумент3 страницыDrug Study: Pharmacokinetics Absorption SiteCarissa Mae Tapec EstradaОценок пока нет
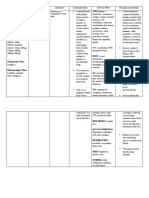
- Drug Classification Action Indication Contraindication Nursing ResposibilitiesДокумент10 страницDrug Classification Action Indication Contraindication Nursing ResposibilitiesAngelicaОценок пока нет
- Drug Study - Morphine (Sulfate)Документ3 страницыDrug Study - Morphine (Sulfate)Kian Herrera100% (2)
- Drug Study - MorphineДокумент3 страницыDrug Study - MorphineKian HerreraОценок пока нет
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingДокумент1 страницаAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12Оценок пока нет
- Pain Medication TableДокумент3 страницыPain Medication TableBruno FernandesОценок пока нет
- Pain Medication TableДокумент3 страницыPain Medication TableRobert ChristevenОценок пока нет
- Pain Medication TableДокумент3 страницыPain Medication TableAsia GobourneОценок пока нет
- Onset, Peak and Duration of Common Pain MedicationsДокумент3 страницыOnset, Peak and Duration of Common Pain MedicationsDwiОценок пока нет
- Pain Medication TableДокумент3 страницыPain Medication TableRobert ChristevenОценок пока нет
- Morphine (Astramorph) PCAДокумент2 страницыMorphine (Astramorph) PCAAdrianne Bazo100% (3)
- Buotan Si June Buotan Jud Si JuneДокумент13 страницBuotan Si June Buotan Jud Si JuneMajestic RavenОценок пока нет
- AminophyllineДокумент3 страницыAminophyllineAmna Kazmi ShehzadОценок пока нет
- PDF Drug Study Morphine SulfateДокумент3 страницыPDF Drug Study Morphine SulfateCrishelОценок пока нет
- Morphine Drug StudyДокумент3 страницыMorphine Drug StudyXerxes Dejito100% (2)
- PromethazineДокумент3 страницыPromethazineGwyn RosalesОценок пока нет
- Drug Study 1Документ2 страницыDrug Study 1Hafza MacabatoОценок пока нет
- Drug Study (Haloperidol)Документ3 страницыDrug Study (Haloperidol)Mae Ann Bueno CastillonОценок пока нет
- Drug StudyДокумент11 страницDrug StudyAlex cyyyОценок пока нет
- GuaifenesinДокумент2 страницыGuaifenesincoooleОценок пока нет
- Ectopic Pregnancy CasiaДокумент16 страницEctopic Pregnancy CasiaMarie Ashley CasiaОценок пока нет
- 9 PropofolДокумент2 страницы9 PropofolAbdelhafiz Susmiran100% (3)
- Aerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaДокумент4 страницыAerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaGwyn RosalesОценок пока нет
- Dosage: 50 MG Order: PRN q6h Route: IV (Case Scenario Based)Документ3 страницыDosage: 50 MG Order: PRN q6h Route: IV (Case Scenario Based)Edward Luis EsguerraОценок пока нет
- FentanylДокумент2 страницыFentanylKatie McPeek63% (8)
- Drug Study: Atropine: RecommendedДокумент6 страницDrug Study: Atropine: RecommendedShara Lailanie A. AzisОценок пока нет
- 8 Propofol Drug StudyДокумент4 страницы8 Propofol Drug Studyshadow gonzalez100% (1)
- Drug Study #3Документ8 страницDrug Study #3James Emman ClementeОценок пока нет
- Brand Name: Chemical Effect: CNS: DizzinessДокумент2 страницыBrand Name: Chemical Effect: CNS: DizzinessGwww BabababaОценок пока нет
- MeclizineДокумент2 страницыMeclizineGwyn Rosales100% (1)
- Vicodin Drug Study Que Fransis A.Документ3 страницыVicodin Drug Study Que Fransis A.Irene Grace BalcuevaОценок пока нет
- Drug Study: Adult: Induction: 40 MGДокумент2 страницыDrug Study: Adult: Induction: 40 MGpretty_mary100% (4)
- MC HydroxyzineДокумент3 страницыMC HydroxyzineCliff by the seaОценок пока нет
- Ipratroprium Drug CardДокумент3 страницыIpratroprium Drug CardXiaoDuckyОценок пока нет
- Postoperative Pain Management Doc 7648Документ8 страницPostoperative Pain Management Doc 7648Muthuvigneswaran ChidambaranathanОценок пока нет
- PrednisoneДокумент3 страницыPrednisoneShaira TanОценок пока нет
- AcetaminophenДокумент3 страницыAcetaminophenShaira Tan100% (1)
- Risperidone Drug StudyДокумент2 страницыRisperidone Drug StudyBasema HashhashОценок пока нет
- Drug StudyДокумент186 страницDrug StudyTheresa Sombilla FacunlaОценок пока нет
- Drug StudyДокумент12 страницDrug StudyHannah DuyagОценок пока нет
- DRUG STUDY - Delos SantosДокумент1 страницаDRUG STUDY - Delos SantosJulia Rae Delos SantosОценок пока нет
- Nausea and Vomiting Nausea and VomitingДокумент6 страницNausea and Vomiting Nausea and VomitingTHERESA CLAIRE ENCINARESОценок пока нет
- Drug Study SalbutamolДокумент2 страницыDrug Study Salbutamolliza sian100% (2)
- Drug Study: Davao Doctor College Nursing ProgramДокумент3 страницыDrug Study: Davao Doctor College Nursing Programember parkОценок пока нет
- Drug Study: Pharmacokinetic S Absorption SiteДокумент4 страницыDrug Study: Pharmacokinetic S Absorption SiteCarissa Mae Tapec EstradaОценок пока нет
- 20 - Obstetrical Analgesia and AnesthesiaДокумент9 страниц20 - Obstetrical Analgesia and AnesthesiaGen XОценок пока нет
- Medications: Medication Name Generic/Trade Classification Pregnancy CategoryДокумент8 страницMedications: Medication Name Generic/Trade Classification Pregnancy CategoryapalestiОценок пока нет
- PSD Quiz#1Документ12 страницPSD Quiz#1yogita marsoniaОценок пока нет
- Propanolol Methimazole Drug StudyДокумент8 страницPropanolol Methimazole Drug Studyheckin meiОценок пока нет
- TRAMADOLДокумент2 страницыTRAMADOLchristine mercadoОценок пока нет
- Drug Study Pre OpДокумент6 страницDrug Study Pre OpgiaОценок пока нет
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingДокумент1 страницаAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12Оценок пока нет
- Morphine (Astramorph)Документ1 страницаMorphine (Astramorph)Adrianne BazoОценок пока нет
- Drug StudyДокумент38 страницDrug StudyRobie Rosa TabagoyОценок пока нет
- Related Readings: N OR S UДокумент3 страницыRelated Readings: N OR S UApple MaeОценок пока нет
- 19a-Reading 1Документ28 страниц19a-Reading 1Apple MaeОценок пока нет
- Human Vaccines & Immunotherapeutics: Yong Liu, Xichao Mo, Xiaxia Yu, Jinxin Wang, Jinfei Tian, Jun Kuang & Jie PengДокумент10 страницHuman Vaccines & Immunotherapeutics: Yong Liu, Xichao Mo, Xiaxia Yu, Jinxin Wang, Jinfei Tian, Jun Kuang & Jie PengApple MaeОценок пока нет
- Human Vaccines & Immunotherapeutics: Yong Liu, Xichao Mo, Xiaxia Yu, Jinxin Wang, Jinfei Tian, Jun Kuang & Jie PengДокумент10 страницHuman Vaccines & Immunotherapeutics: Yong Liu, Xichao Mo, Xiaxia Yu, Jinxin Wang, Jinfei Tian, Jun Kuang & Jie PengApple MaeОценок пока нет
- N OR S U: Egros Iental Tate NiversityДокумент2 страницыN OR S U: Egros Iental Tate NiversityApple MaeОценок пока нет
- 10b-Discussion of The DiseaseДокумент7 страниц10b-Discussion of The DiseaseApple MaeОценок пока нет
- N OR S U: Egros Iental Tate NiversityДокумент1 страницаN OR S U: Egros Iental Tate NiversityApple MaeОценок пока нет
- God 2. Health 3. Family 4. Relationship 5. Love 6. Friends 7. Peace 8. Self-Development 9. Career 10. MoneyДокумент3 страницыGod 2. Health 3. Family 4. Relationship 5. Love 6. Friends 7. Peace 8. Self-Development 9. Career 10. MoneyApple MaeОценок пока нет
- Sample Presentation ScriptДокумент3 страницыSample Presentation ScriptApple MaeОценок пока нет
- 8-Growth & DevelopmentДокумент1 страница8-Growth & DevelopmentApple MaeОценок пока нет
- Medical Management (Schizophrenia)Документ5 страницMedical Management (Schizophrenia)Apple MaeОценок пока нет
- 10a-Discussion of The DiseaseДокумент5 страниц10a-Discussion of The DiseaseApple MaeОценок пока нет
- N OR S U: Egros Iental Tate NiversityДокумент2 страницыN OR S U: Egros Iental Tate NiversityApple MaeОценок пока нет
- Dissociative DisordersДокумент17 страницDissociative Disordersapi-3797941100% (4)
- Antipsychotic Drugs: Conventional AntipsychoticsДокумент16 страницAntipsychotic Drugs: Conventional AntipsychoticsApple MaeОценок пока нет
- Pathophysiology of Dengue FeverДокумент1 страницаPathophysiology of Dengue FeverApple Mae100% (1)
- VITAMIN-E and KДокумент4 страницыVITAMIN-E and KApple MaeОценок пока нет
- N OR S U: Clinical DataДокумент2 страницыN OR S U: Clinical DataApple MaeОценок пока нет
- N OR S U: Egros Iental Tate NiversityДокумент2 страницыN OR S U: Egros Iental Tate NiversityApple MaeОценок пока нет
- Minor OR (Notes)Документ11 страницMinor OR (Notes)Apple MaeОценок пока нет
- Scenario Liver Cirrhosis Stage 2Документ1 страницаScenario Liver Cirrhosis Stage 2Apple MaeОценок пока нет
- Nursing ManagementДокумент1 страницаNursing ManagementApple MaeОценок пока нет
- Major Duties For Same-Day SurgeryДокумент1 страницаMajor Duties For Same-Day SurgeryApple MaeОценок пока нет
- PopsicleДокумент2 страницыPopsicleApple MaeОценок пока нет
- Covid-19 Faqs: Last Updated: 2 March 2020Документ6 страницCovid-19 Faqs: Last Updated: 2 March 2020Apple MaeОценок пока нет
- I. Cutting and DissectingДокумент10 страницI. Cutting and DissectingApple MaeОценок пока нет
- Minor Surgery Is Defines As A Set of Procedures in Which Short Surgical Techniques Are Applied OnДокумент11 страницMinor Surgery Is Defines As A Set of Procedures in Which Short Surgical Techniques Are Applied OnApple MaeОценок пока нет
- Pre and Post TestДокумент4 страницыPre and Post TestApple MaeОценок пока нет
- Wound CareДокумент6 страницWound CareApple MaeОценок пока нет
- 16-Skin Safety and Health Prevention An Overview of Chemicals in Cosmetic Products (2019) PDFДокумент8 страниц16-Skin Safety and Health Prevention An Overview of Chemicals in Cosmetic Products (2019) PDFApple MaeОценок пока нет
- Reaction PaperДокумент3 страницыReaction PaperCecille Robles San JoseОценок пока нет
- Resume Testing6+ SaptagireswarДокумент5 страницResume Testing6+ SaptagireswarSuresh RamasamyОценок пока нет
- STEM BeesДокумент36 страницSTEM BeesHitesh YadavОценок пока нет
- Malefactor ClassДокумент23 страницыMalefactor ClassMatthew Duncan100% (6)
- Marketing Plan For Paraiso Islet ResortДокумент25 страницMarketing Plan For Paraiso Islet ResortEllaine Claire Lor100% (1)
- Broshure JepanДокумент6 страницBroshure JepanIrwan Mohd YusofОценок пока нет
- Ylarde vs. Aquino, GR 33722 (DIGEST)Документ1 страницаYlarde vs. Aquino, GR 33722 (DIGEST)Lourdes Loren Cruz67% (3)
- Ross, D. (2013) - Field Guide To Jumping Spiders of Southeast Idaho.Документ4 страницыRoss, D. (2013) - Field Guide To Jumping Spiders of Southeast Idaho.Dave RossОценок пока нет
- PED100 Mod2Документ3 страницыPED100 Mod2Risa BarritaОценок пока нет
- AS 1 Pretest TOS S.Y. 2018-2019Документ2 страницыAS 1 Pretest TOS S.Y. 2018-2019Whilmark Tican MucaОценок пока нет
- Nin/Pmjay Id Name of The Vaccination Site Category Type District BlockДокумент2 страницыNin/Pmjay Id Name of The Vaccination Site Category Type District BlockNikunja PadhanОценок пока нет
- Biometric Security ConcernsДокумент27 страницBiometric Security ConcernsprinceuchenduОценок пока нет
- Mathematicaleconomics PDFДокумент84 страницыMathematicaleconomics PDFSayyid JifriОценок пока нет
- Openfire XXMPP Server On Windows Server 2012 R2Документ9 страницOpenfire XXMPP Server On Windows Server 2012 R2crobertoОценок пока нет
- Character Formation 1: Nationalism and PatriotismДокумент11 страницCharacter Formation 1: Nationalism and Patriotismban diaz100% (1)
- Flow ChemistryДокумент6 страницFlow Chemistryrr1819Оценок пока нет
- Symbiosis National Aptitude Test (SNAP) 2004: InstructionsДокумент21 страницаSymbiosis National Aptitude Test (SNAP) 2004: InstructionsHarsh JainОценок пока нет
- Case - Marico SCMДокумент26 страницCase - Marico SCMChandan Gupta50% (2)
- Direct Filter Synthesis Rhea PreviewДокумент25 страницDirect Filter Synthesis Rhea Previewoprakash9291Оценок пока нет
- Acidity (As Acetic Acid) On Undenatured and Denatured EthanolДокумент10 страницAcidity (As Acetic Acid) On Undenatured and Denatured EthanolVinh NguyenОценок пока нет
- Engineering Road Note 9 - May 2012 - Uploaded To Main Roads Web SiteДокумент52 страницыEngineering Road Note 9 - May 2012 - Uploaded To Main Roads Web SiteRahma SariОценок пока нет
- Binding of IsaacДокумент10 страницBinding of IsaacBraz SouzaОценок пока нет
- Sri Guru Parampara Stotram CompressДокумент14 страницSri Guru Parampara Stotram CompressSatishPavurayalaОценок пока нет
- Navamsa Karma and GodДокумент9 страницNavamsa Karma and GodVisti Larsen50% (2)
- CV AmosДокумент4 страницыCV Amoscharity busoloОценок пока нет
- Amtek Auto Analysis AnuragДокумент4 страницыAmtek Auto Analysis AnuraganuragОценок пока нет
- Ernesto Sirolli - Eenterprise FacilitationДокумент300 страницErnesto Sirolli - Eenterprise FacilitationFrancis James Leite Marques PereiraОценок пока нет
- Oedogonium: Class: Chlorophyceae Order: Oedogoniales Family: OedogoniaceaeДокумент28 страницOedogonium: Class: Chlorophyceae Order: Oedogoniales Family: OedogoniaceaeA SASIKALAОценок пока нет
- Rectification or Correction of Sale DeedДокумент4 страницыRectification or Correction of Sale Deedsumanth_0678Оценок пока нет
- India Marine Insurance Act 1963Документ21 страницаIndia Marine Insurance Act 1963Aman GroverОценок пока нет
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (28)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (81)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningОт EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningРейтинг: 4 из 5 звезд4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Оценок пока нет
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (4)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (170)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Gut: the new and revised Sunday Times bestsellerОт EverandGut: the new and revised Sunday Times bestsellerРейтинг: 4 из 5 звезд4/5 (393)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingОт EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingРейтинг: 4 из 5 звезд4/5 (1138)
- The Marshmallow Test: Mastering Self-ControlОт EverandThe Marshmallow Test: Mastering Self-ControlРейтинг: 4.5 из 5 звезд4.5/5 (58)