Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Pharm Phlash! Pharmacology Flash CardsДокумент206 страницPharm Phlash! Pharmacology Flash Cardsnoname1919154% (26)
- Depression and Mood - ExamineДокумент2 страницыDepression and Mood - ExamineAnonymous RdHoBDhRОценок пока нет
- Medical EthicsДокумент21 страницаMedical EthicsRoan Dones Delos SantosОценок пока нет
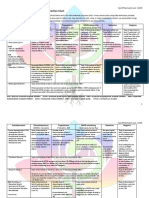
- Antidepressant & Psychedelic Drug Interaction ChartДокумент3 страницыAntidepressant & Psychedelic Drug Interaction ChartFred The Nomad100% (2)
- Psych MedicationsДокумент5 страницPsych MedicationsKalesha Jones100% (2)
- Chapter 21 Antidepressant AgentsДокумент4 страницыChapter 21 Antidepressant AgentsNicolle Lisay IlaganОценок пока нет
- Chapter 2 - Neurobiologic Theories and PsychopharmacologyДокумент11 страницChapter 2 - Neurobiologic Theories and PsychopharmacologyCatia FernandesОценок пока нет
- Transcript of "Jim Kwik: Speed Reading, Memory, & Superlearning - #189"Документ20 страницTranscript of "Jim Kwik: Speed Reading, Memory, & Superlearning - #189"mufabo100% (1)
- CongenitalДокумент25 страницCongenitalSUTHANОценок пока нет
- Ethics Primer 4-17Документ85 страницEthics Primer 4-17Roan Dones Delos SantosОценок пока нет
- China Asia Vision 6Документ5 страницChina Asia Vision 6Roan Dones Delos SantosОценок пока нет
- HTLV I AssociatedДокумент13 страницHTLV I AssociatedRoan Dones Delos SantosОценок пока нет
- DMJ 2020 0258Документ17 страницDMJ 2020 0258Elena Borş MorariОценок пока нет
- Obesity Obesity Management in AdultsДокумент12 страницObesity Obesity Management in AdultsLorena IbarrolaОценок пока нет
- QR CPG TobacoDisorderДокумент8 страницQR CPG TobacoDisorderiman14Оценок пока нет
- Catholic Faith: Clinical Worksheet: Nursing Process Care PlanДокумент18 страницCatholic Faith: Clinical Worksheet: Nursing Process Care Planmuhammad adilОценок пока нет
- Smoking Cessation: Prepared by Dr. Ahmed El MasryДокумент77 страницSmoking Cessation: Prepared by Dr. Ahmed El Masryاحمد المصرىОценок пока нет
- Postpartum Psychiatric DisordersДокумент10 страницPostpartum Psychiatric DisordersRey Mart OrtegaОценок пока нет
- Spirit Pharmacist - Antidepressants and Psychedelics Interactions Tapering GuideДокумент77 страницSpirit Pharmacist - Antidepressants and Psychedelics Interactions Tapering GuideDorotaОценок пока нет
- Quit SmokingДокумент44 страницыQuit SmokingTbwc UmiОценок пока нет
- Non Medical Prescribing Using The British National Formulary PDFДокумент6 страницNon Medical Prescribing Using The British National Formulary PDFRyan MwОценок пока нет
- VIRADAY Tablets (Efavirenz + Emtricitabine + Tenofovir Disoproxil Fumarate)Документ23 страницыVIRADAY Tablets (Efavirenz + Emtricitabine + Tenofovir Disoproxil Fumarate)Revina BustamiОценок пока нет
- HES-005-Session-9-SASДокумент9 страницHES-005-Session-9-SASDave Ortiz Robert MaglasangОценок пока нет
- Slide PsychiatryДокумент28 страницSlide Psychiatryandirio7486Оценок пока нет
- Clinical Guideline 1Документ10 страницClinical Guideline 1klysmanu93Оценок пока нет
- Edward Teach MD - The Last PsychiatristДокумент3 437 страницEdward Teach MD - The Last PsychiatristAugie100% (1)
- Tarea 6. BioestadisticaДокумент7 страницTarea 6. BioestadisticaLuis Reyes VelázquezОценок пока нет
- Adult ADHD - What Do When Your First Drug Fails - Dr.-James-LazowskiДокумент77 страницAdult ADHD - What Do When Your First Drug Fails - Dr.-James-LazowskiJason WongОценок пока нет
- Psych DrugsДокумент3 страницыPsych DrugsSwarna BanikОценок пока нет
- ABCs of Psychiatric MedicinesДокумент41 страницаABCs of Psychiatric Medicines아이닠텓Оценок пока нет
- Cardiology IIДокумент79 страницCardiology IIAhmad MakhloufОценок пока нет
- Mental Health PharmacologicalДокумент6 страницMental Health PharmacologicalKyla Mae De GraciaОценок пока нет
- Internet Addiction and Its Cognitive Behavioral Therapy: Ömer Şenormancı, Ramazan Konkan and Mehmet Zihni SungurДокумент21 страницаInternet Addiction and Its Cognitive Behavioral Therapy: Ömer Şenormancı, Ramazan Konkan and Mehmet Zihni SungurShari' Si WahyuОценок пока нет
- Documentation in Psychiatric NursingДокумент25 страницDocumentation in Psychiatric NursingMichelle ErikaОценок пока нет
- Bupropion and Other Non-Nicotine PharmacotherapiesДокумент3 страницыBupropion and Other Non-Nicotine PharmacotherapiesEstigma Universidad Del RosarioОценок пока нет
- Antidepressants UpdateДокумент24 страницыAntidepressants Updatedrsayis2Оценок пока нет