Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Rhythm Control Versus Rate Control in Atrial FibrillationДокумент22 страницыRhythm Control Versus Rate Control in Atrial FibrillationAnca StanОценок пока нет
- Overview of Atrial Flutter: Authors: Section Editor: Deputy EditorДокумент20 страницOverview of Atrial Flutter: Authors: Section Editor: Deputy EditorAnca StanОценок пока нет
- Sustained Monomorphic Ventricular Tachycardia in Patients With Structural Heart Disease: Treatment and PrognosisДокумент25 страницSustained Monomorphic Ventricular Tachycardia in Patients With Structural Heart Disease: Treatment and PrognosisAnca StanОценок пока нет
- Reentry and The Development of Cardiac Arrhythmias: Author: Section Editor: Deputy EditorДокумент36 страницReentry and The Development of Cardiac Arrhythmias: Author: Section Editor: Deputy EditorAnca StanОценок пока нет
- Prognosis and Outcomes Following Sudden Cardiac Arrest in AdultsДокумент24 страницыPrognosis and Outcomes Following Sudden Cardiac Arrest in AdultsAnca StanОценок пока нет
- Pathophysiology and Etiology of Sudden Cardiac Arrest: Author: Section Editors: Deputy EditorДокумент23 страницыPathophysiology and Etiology of Sudden Cardiac Arrest: Author: Section Editors: Deputy EditorAnca StanОценок пока нет
- Secondary Prevention of Sudden Cardiac Death in Heart Failure and CardiomyopathyДокумент24 страницыSecondary Prevention of Sudden Cardiac Death in Heart Failure and CardiomyopathyAnca StanОценок пока нет
- Paroxysmal Atrial FibrillationДокумент14 страницParoxysmal Atrial FibrillationAnca StanОценок пока нет
- Implantable Cardioverter-Defibrillators: Optimal ProgrammingДокумент29 страницImplantable Cardioverter-Defibrillators: Optimal ProgrammingAnca StanОценок пока нет
- New Onset Atrial FibrillationДокумент15 страницNew Onset Atrial FibrillationAnca StanОценок пока нет
- Implantable Cardioverter-Defibrillators: Overview of Indications, Components, and FunctionsДокумент23 страницыImplantable Cardioverter-Defibrillators: Overview of Indications, Components, and FunctionsAnca StanОценок пока нет
- Overview of Atrial Fibrillation: "The Electrocardiogram in Atrial Fibrillation", Section On 'Common Findings'Документ28 страницOverview of Atrial Fibrillation: "The Electrocardiogram in Atrial Fibrillation", Section On 'Common Findings'Anca StanОценок пока нет
- 4 5931499803149076504 PDFДокумент126 страниц4 5931499803149076504 PDFCristianAltunaSotomayorОценок пока нет
- Disseminated Intravascular Coagulation (DIC) in Adults: Evaluation and ManagementДокумент46 страницDisseminated Intravascular Coagulation (DIC) in Adults: Evaluation and ManagementAnca StanОценок пока нет
- Arrhythmia-Induced Cardiomyopathy - UpToDateДокумент30 страницArrhythmia-Induced Cardiomyopathy - UpToDateAnca StanОценок пока нет
- Endovascular Repair of The Thoracic Aorta - UpToDateДокумент48 страницEndovascular Repair of The Thoracic Aorta - UpToDateAnca StanОценок пока нет
- Cardiovascular Benefits and Risks of Moderate Alcohol Consumption - UpToDateДокумент17 страницCardiovascular Benefits and Risks of Moderate Alcohol Consumption - UpToDateAnca StanОценок пока нет
- Differentiating Constrictive Pericarditis and Restrictive Cardiomyopathy - UpToDateДокумент3 страницыDifferentiating Constrictive Pericarditis and Restrictive Cardiomyopathy - UpToDateAnca StanОценок пока нет
- Definition and Classification of The Cardiomyopathies - UpToDateДокумент39 страницDefinition and Classification of The Cardiomyopathies - UpToDateAnca StanОценок пока нет
- Alcoholic Cardiomyopathy - UpToDateДокумент29 страницAlcoholic Cardiomyopathy - UpToDateAnca StanОценок пока нет
- Late Recurrent Angina Pectoris After Coronary Artery Bypass Graft Surgery - UpToDateДокумент16 страницLate Recurrent Angina Pectoris After Coronary Artery Bypass Graft Surgery - UpToDateAnca StanОценок пока нет
- Complications of Endovascular Abdominal Aortic Repair - UpToDateДокумент38 страницComplications of Endovascular Abdominal Aortic Repair - UpToDateAnca StanОценок пока нет
- Abdominal Vascular Injury - UpToDateДокумент3 страницыAbdominal Vascular Injury - UpToDateAnca StanОценок пока нет
- Early Noncardiac Complications of Coronary Artery Bypass Graft Surgery - UpToDateДокумент37 страницEarly Noncardiac Complications of Coronary Artery Bypass Graft Surgery - UpToDateAnca StanОценок пока нет
- Early Cardiac Complications of Coronary Artery Bypass Graft Surgery - UpToDateДокумент16 страницEarly Cardiac Complications of Coronary Artery Bypass Graft Surgery - UpToDateAnca StanОценок пока нет
- Evaluation of Emergency Department Patients With Chest Pain at Low or Intermediate Risk For Acute Coronary Syndrome - UpToDateДокумент29 страницEvaluation of Emergency Department Patients With Chest Pain at Low or Intermediate Risk For Acute Coronary Syndrome - UpToDateAnca StanОценок пока нет
- Coronary Artery Stent Thrombosis - Clinical Presentation and Management - UpToDateДокумент13 страницCoronary Artery Stent Thrombosis - Clinical Presentation and Management - UpToDateAnca StanОценок пока нет
- Coronary Endothelial Dysfunction - Clinical Aspects - UpToDateДокумент29 страницCoronary Endothelial Dysfunction - Clinical Aspects - UpToDateAnca StanОценок пока нет
- Coronary Artery Revascularization in Stable Patients With Diabetes Mellitus - UpToDateДокумент22 страницыCoronary Artery Revascularization in Stable Patients With Diabetes Mellitus - UpToDateAnca StanОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Malaria SymptomsДокумент3 страницыMalaria SymptomsShaula de OcampoОценок пока нет
- Government of Kerala: Minority CertificateДокумент1 страницаGovernment of Kerala: Minority CertificateBI185824125 Personal AccountingОценок пока нет
- Lesson 6 S and V AgreementДокумент6 страницLesson 6 S and V AgreementLinh Ngọc NguyễnОценок пока нет
- PrinciplesIntuitiveEating2017 PDFДокумент2 страницыPrinciplesIntuitiveEating2017 PDFCristina Cousinard100% (2)
- How To Effectively CommunicateДокумент44 страницыHow To Effectively CommunicatetaapОценок пока нет
- GrandEsta - Double Eyelid Surgery PDFДокумент2 страницыGrandEsta - Double Eyelid Surgery PDFaniyaОценок пока нет
- Mission Veng 29th, 2019Документ4 страницыMission Veng 29th, 2019Lasky ChhakchhuakОценок пока нет
- Chapter-British Parliamentary Debate FormatДокумент8 страницChapter-British Parliamentary Debate FormatNoelle HarrisonОценок пока нет
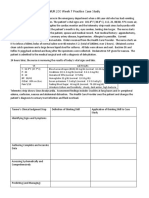
- NUR 200 Week 7 Practice Case StudyДокумент2 страницыNUR 200 Week 7 Practice Case StudyJB NicoleОценок пока нет
- Security and Azure SQL Database White PaperДокумент15 страницSecurity and Azure SQL Database White PaperSteve SmithОценок пока нет
- Villa VeronicaДокумент12 страницVilla Veronicacj fontzОценок пока нет
- Fundamentals of Biochemical Engineering Dutta Solution ManualДокумент6 страницFundamentals of Biochemical Engineering Dutta Solution Manualhimanshu18% (22)
- Computerized Dynamic Posturography (CDP)Документ2 страницыComputerized Dynamic Posturography (CDP)eldescribdОценок пока нет
- Chapter 2 - Professinal Ethics Legal LiabilityДокумент29 страницChapter 2 - Professinal Ethics Legal LiabilityThị Hải Yến TrầnОценок пока нет
- Swimming Pool - PWTAG CodeofPractice1.13v5 - 000Документ58 страницSwimming Pool - PWTAG CodeofPractice1.13v5 - 000Vin BdsОценок пока нет
- Assignment 1 TVM, Bonds StockДокумент2 страницыAssignment 1 TVM, Bonds StockMuhammad Ali SamarОценок пока нет
- Remo Vs DevanaderaДокумент2 страницыRemo Vs DevanaderaZymon Andrew MaquintoОценок пока нет
- Ethics - FinalsДокумент18 страницEthics - Finalsannie lalangОценок пока нет
- HotsДокумент74 страницыHotsgecko195Оценок пока нет
- Live Leak - SSC CGL Tier II English Model Question Paper (Based On Predicted Pattern 2016)Документ44 страницыLive Leak - SSC CGL Tier II English Model Question Paper (Based On Predicted Pattern 2016)Testbook BlogОценок пока нет
- Case Study Beta Management Company: Raman Dhiman Indian Institute of Management (Iim), ShillongДокумент8 страницCase Study Beta Management Company: Raman Dhiman Indian Institute of Management (Iim), ShillongFabián Fuentes100% (1)
- Equilibrium of Firm Under Perfect Competition: Presented by Piyush Kumar 2010EEE023Документ18 страницEquilibrium of Firm Under Perfect Competition: Presented by Piyush Kumar 2010EEE023a0mittal7Оценок пока нет
- GCF and LCMДокумент34 страницыGCF and LCMНикому Не Известный ЧеловекОценок пока нет
- The American New CriticsДокумент5 страницThe American New CriticsSattigul KharakozhaОценок пока нет
- The Main Ideas in An Apology For PoetryДокумент6 страницThe Main Ideas in An Apology For PoetryShweta kashyap100% (3)
- Accounting For Employee Stock OptionsДокумент22 страницыAccounting For Employee Stock OptionsQuant TradingОценок пока нет
- Formulating A PICOT QuestionДокумент4 страницыFormulating A PICOT QuestionKarl RobleОценок пока нет
- F A T City Workshop NotesДокумент3 страницыF A T City Workshop Notesapi-295119035Оценок пока нет
- Upanikhat-I Garbha A Mughal Translation PDFДокумент18 страницUpanikhat-I Garbha A Mughal Translation PDFReginaldoJurandyrdeMatosОценок пока нет
- Cluster of Business and Management: BBAW 2103 Financial AccountingДокумент13 страницCluster of Business and Management: BBAW 2103 Financial AccountingFreshlynero JonalОценок пока нет