Вам также может понравиться
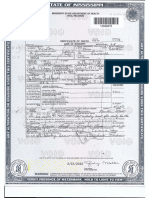
- Certificate of DeathДокумент2 страницыCertificate of DeathAngel Urbano67% (3)
- Analysis of Electric Machinery Krause Manual Solution PDFДокумент2 страницыAnalysis of Electric Machinery Krause Manual Solution PDFKuldeep25% (8)
- Manual s10 PDFДокумент402 страницыManual s10 PDFLibros18Оценок пока нет
- 1833 TX Melton, Daisy Mae DeathДокумент1 страница1833 TX Melton, Daisy Mae DeathRichard TonsingОценок пока нет
- Img 0001Документ1 страницаImg 0001alex vitalicio100% (1)
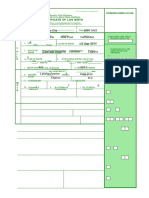
- Birth CertificateДокумент4 страницыBirth CertificateJhaymie MagsailОценок пока нет
- Sample: Oncotype DX Breast Cancer AssayДокумент2 страницыSample: Oncotype DX Breast Cancer Assaybirhane gebreegziabiherОценок пока нет
- 70 Valves SolenoidДокумент105 страниц70 Valves SolenoidrizalОценок пока нет
- Abiera Final FileДокумент81 страницаAbiera Final FileDeo Montero OrquejoОценок пока нет
- Excon2019 ShowPreview02122019 PDFДокумент492 страницыExcon2019 ShowPreview02122019 PDFSanjay KherОценок пока нет
- Main Municipal Form 103 Certificate Death CatbqaloganДокумент3 страницыMain Municipal Form 103 Certificate Death CatbqaloganNoriel SarmientoОценок пока нет
- Img 20191219 0001Документ1 страницаImg 20191219 0001KIMBERLY BALISACANОценок пока нет
- Certificate of Death: Office of The Civil Register GeneralДокумент3 страницыCertificate of Death: Office of The Civil Register Generalbktsuna0201Оценок пока нет
- BionoteДокумент4 страницыBionoteAngela Neri100% (1)
- Benevisión N15 Mindray Service ManualДокумент123 страницыBenevisión N15 Mindray Service ManualSulay Avila LlanosОценок пока нет
- Unified Multl-Purpose Id (Umid) Card Application: D D D DДокумент3 страницыUnified Multl-Purpose Id (Umid) Card Application: D D D Djanel norbeОценок пока нет
- HEMS Form 3-A - Oct. 23, 2010 (As of 3 PM)Документ2 страницыHEMS Form 3-A - Oct. 23, 2010 (As of 3 PM)Umm MiyaasaОценок пока нет
- BritДокумент1 страницаBritCheryl CabanzaОценок пока нет
- Form Application RonquillomarlendДокумент1 страницаForm Application RonquillomarlendMarlen RonquilloОценок пока нет
- Birth Cert LalaineДокумент2 страницыBirth Cert LalaineGerry Boy BailonОценок пока нет
- UntitledДокумент24 страницыUntitledalex estavОценок пока нет
- Certificate of Live Birth Form PhilippinesДокумент3 страницыCertificate of Live Birth Form PhilippinesGerry Boy BailonОценок пока нет
- Capd 000001051Документ4 страницыCapd 000001051Capitol Breach DiscoveryОценок пока нет
- 20200727082947WEHU-A1A2 - Occupational Accident and Dangerous OccurrenceДокумент3 страницы20200727082947WEHU-A1A2 - Occupational Accident and Dangerous OccurrenceNORASHIDA BT ABU HASSAN (MOH)Оценок пока нет
- Formmed Rev3Документ2 страницыFormmed Rev3RR Sasmaya HatiОценок пока нет
- Stecco Ficha AnamneseДокумент2 страницыStecco Ficha AnamneseRobson SenaОценок пока нет
- Mo Ve Pa Ve: Segments Locat Side Durat (Acu-1°) T/? Si Pa Pa Conc Extremit. Pa Prev Surgery Trauma FractureДокумент2 страницыMo Ve Pa Ve: Segments Locat Side Durat (Acu-1°) T/? Si Pa Pa Conc Extremit. Pa Prev Surgery Trauma FractureRobson SenaОценок пока нет
- Disaster Victim Identification (Dvi) : ( (GB) Version 2008)Документ21 страницаDisaster Victim Identification (Dvi) : ( (GB) Version 2008)Fikri RozanОценок пока нет
- Staffing For Doc On TV MedДокумент3 страницыStaffing For Doc On TV MedADD Foundation PolyclinicОценок пока нет
- VAW Form 1Документ1 страницаVAW Form 1Angela TabudlongОценок пока нет
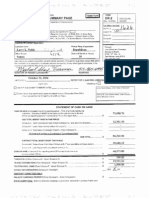
- Disclosure Summary Page DR-2: Noble For SenateДокумент10 страницDisclosure Summary Page DR-2: Noble For SenateZach EdwardsОценок пока нет
- CP FormsДокумент12 страницCP FormsLovely Pescante CuananОценок пока нет
- CHN Survey NewДокумент3 страницыCHN Survey NewEvelyn BuenОценок пока нет
- Medical History ReportДокумент4 страницыMedical History ReportRacel AbulaОценок пока нет
- SSSForms UMID ApplicationДокумент2 страницыSSSForms UMID ApplicationhazelnutdesuОценок пока нет
- Rha Municipal Consolidation'Документ3 страницыRha Municipal Consolidation'D Alfz EinsTein JDОценок пока нет
- Cert of Death Tobe FalknerДокумент1 страницаCert of Death Tobe Falknerras rahmaniОценок пока нет
- New Ltia Forms 6 7BДокумент17 страницNew Ltia Forms 6 7BkatedestrizaОценок пока нет
- Borang Pemeriksaan-Mammografi 1Документ2 страницыBorang Pemeriksaan-Mammografi 1hsentosaoshОценок пока нет
- Peme Form - NepiaДокумент3 страницыPeme Form - Nepiamakssirodchuk10Оценок пока нет
- POSTAL - Application Mikey. ANSWERДокумент2 страницыPOSTAL - Application Mikey. ANSWERAmy DartОценок пока нет
- Capd 000001115Документ4 страницыCapd 000001115Capitol Breach DiscoveryОценок пока нет
- Eom 2018 00025Документ256 страницEom 2018 00025radeobaldiaОценок пока нет
- KerneraДокумент31 страницаKerneraapi-643855788Оценок пока нет
- Capd 000001101Документ4 страницыCapd 000001101Capitol Breach DiscoveryОценок пока нет
- Capd 000001075Документ4 страницыCapd 000001075Capitol Breach DiscoveryОценок пока нет
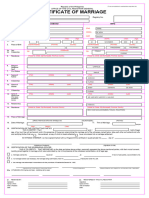
- Form No 97 MarriageДокумент2 страницыForm No 97 Marriageimeldatiano16Оценок пока нет
- Pid Application FormДокумент2 страницыPid Application FormTsugumi Kate PulongbaritОценок пока нет
- Annex (1) Health Check-Up Form: Detailed Candidate ReportДокумент6 страницAnnex (1) Health Check-Up Form: Detailed Candidate ReportMukesh MistriОценок пока нет
- Barangay Data Capture Form Monitoring of Incidence On Violence Against Women (Vaw) During The Covid-19 PandemicДокумент4 страницыBarangay Data Capture Form Monitoring of Incidence On Violence Against Women (Vaw) During The Covid-19 Pandemicbarangay 608Оценок пока нет
- Eastern Washington University Police Report For Racial SlurДокумент5 страницEastern Washington University Police Report For Racial SlurThe College FixОценок пока нет
- PDS and Work Experience Sheet 2021Документ8 страницPDS and Work Experience Sheet 2021melogyОценок пока нет
- Application For Postal Id CardДокумент1 страницаApplication For Postal Id CardRommel AzoresОценок пока нет
- Adobe Scan Aug 06, 2021Документ2 страницыAdobe Scan Aug 06, 2021Kitty XinОценок пока нет
- Cored SampleДокумент1 страницаCored SampleniixiedomingoОценок пока нет
- Latest 2021 Cs Form No 212 Pds Pro Cabajes 2021Документ35 страницLatest 2021 Cs Form No 212 Pds Pro Cabajes 2021bevlesoyОценок пока нет
- Death Certificate Template 09Документ2 страницыDeath Certificate Template 09david90397Оценок пока нет
- Inbound 7714832539582663562Документ17 страницInbound 7714832539582663562Julesbon ParsaliganОценок пока нет
- Form Jul 27, 2021Документ1 страницаForm Jul 27, 2021Melodie TabuadaОценок пока нет
- OR CommsДокумент4 страницыOR CommsAngela NeriОценок пока нет
- Training Design Iec Material BSN 409 Grp2b SNДокумент17 страницTraining Design Iec Material BSN 409 Grp2b SNAngela NeriОценок пока нет
- Level 4 Modules For Nursing Skills AuditДокумент95 страницLevel 4 Modules For Nursing Skills AuditAngela NeriОценок пока нет
- Impact of A Modified Nursing Handover ModelДокумент9 страницImpact of A Modified Nursing Handover ModelAngela NeriОценок пока нет
- Nle FC Manila 2023 May - EDITEDДокумент12 страницNle FC Manila 2023 May - EDITEDAngela NeriОценок пока нет
- @acelleisboring - NCP Risk For AspirationДокумент6 страниц@acelleisboring - NCP Risk For AspirationAngela NeriОценок пока нет
- @lfnursingcomms - DRUG STUDY FAJARDO ANDREA LAUREN A.Документ6 страниц@lfnursingcomms - DRUG STUDY FAJARDO ANDREA LAUREN A.Angela NeriОценок пока нет
- Sacraments 2Документ68 страницSacraments 2Angela NeriОценок пока нет
- Medication Administration Group 2Документ32 страницыMedication Administration Group 2Angela NeriОценок пока нет
- Typhoon Yunya (1991) - WikipediaДокумент6 страницTyphoon Yunya (1991) - WikipediaAngela NeriОценок пока нет
- What Is Lacking in Us?: What Do You Think We, Human Beings, When We Lack The Sanctifying Grace of ?Документ20 страницWhat Is Lacking in Us?: What Do You Think We, Human Beings, When We Lack The Sanctifying Grace of ?Angela NeriОценок пока нет
- Chan ReferencesДокумент93 страницыChan ReferencesAngela NeriОценок пока нет
- Colonic Mass PathophysioДокумент1 страницаColonic Mass PathophysioAngela NeriОценок пока нет
- Education, by Ellen G. White. Chapter 14 - Science and The BibleДокумент4 страницыEducation, by Ellen G. White. Chapter 14 - Science and The BibleAngela NeriОценок пока нет
- Program Flow DraftДокумент1 страницаProgram Flow DraftAngela NeriОценок пока нет
- Crash Cart Check ListДокумент2 страницыCrash Cart Check ListAngela NeriОценок пока нет
- Training DesignДокумент1 страницаTraining DesignAngela NeriОценок пока нет
- AristotleДокумент7 страницAristotleAngela NeriОценок пока нет
- ReflectivePaper DAY1 NERIДокумент2 страницыReflectivePaper DAY1 NERIAngela NeriОценок пока нет
- Introduction To Physical Fitness: Prepared by Professor Elenita LeabresДокумент11 страницIntroduction To Physical Fitness: Prepared by Professor Elenita LeabresAngela NeriОценок пока нет
- Sample Problem Solving ProcessДокумент5 страницSample Problem Solving ProcessAngela NeriОценок пока нет
- A Social Life in Reality: Facebook From The Funny Memes To Videos That Simply Make Me Laugh. in Observation As Well ToДокумент2 страницыA Social Life in Reality: Facebook From The Funny Memes To Videos That Simply Make Me Laugh. in Observation As Well ToAngela NeriОценок пока нет
- Lactation Common Nutritional Problems and Recommended DietДокумент1 страницаLactation Common Nutritional Problems and Recommended DietAngela NeriОценок пока нет
- FA#2 Essay - NERI (Elderly Health)Документ2 страницыFA#2 Essay - NERI (Elderly Health)Angela NeriОценок пока нет
- Movie Review: "What A Beautiful Mind"Документ4 страницыMovie Review: "What A Beautiful Mind"Angela NeriОценок пока нет
- Group 2B: A Pulmonary Histoplasmosis CaseДокумент58 страницGroup 2B: A Pulmonary Histoplasmosis CaseAngela NeriОценок пока нет
- Angela P. Neri March 4, 2021 BSN 309 Mad Rle Act # 2Документ3 страницыAngela P. Neri March 4, 2021 BSN 309 Mad Rle Act # 2Angela NeriОценок пока нет
- Nutrition of AdolescenceДокумент7 страницNutrition of AdolescenceAngela NeriОценок пока нет
- B122 - Tma03Документ7 страницB122 - Tma03Martin SantambrogioОценок пока нет
- Countries EXCESS DEATHS All Ages - 15nov2021Документ21 страницаCountries EXCESS DEATHS All Ages - 15nov2021robaksОценок пока нет
- Dialogue Au Restaurant, Clients Et ServeurДокумент9 страницDialogue Au Restaurant, Clients Et ServeurbanuОценок пока нет
- SSGC-RSGLEG Draft Study On The Applicability of IAL To Cyber Threats Against Civil AviationДокумент41 страницаSSGC-RSGLEG Draft Study On The Applicability of IAL To Cyber Threats Against Civil AviationPrachita AgrawalОценок пока нет
- De Thi Hoc Ki 1 Mon Tieng Anh Lop 5 Co File NgheДокумент10 страницDe Thi Hoc Ki 1 Mon Tieng Anh Lop 5 Co File Nghetuyen truongОценок пока нет
- Rockaway Times 11818Документ40 страницRockaway Times 11818Peter J. MahonОценок пока нет
- PyhookДокумент23 страницыPyhooktuan tuanОценок пока нет
- Waterstop TechnologyДокумент69 страницWaterstop TechnologygertjaniОценок пока нет
- Work ProblemsДокумент19 страницWork ProblemsOfelia DavidОценок пока нет
- Test ScienceДокумент2 страницыTest Sciencejam syОценок пока нет
- Appendix - Pcmc2Документ8 страницAppendix - Pcmc2Siva PОценок пока нет
- PM CH 14Документ24 страницыPM CH 14phani chowdaryОценок пока нет
- ME Eng 8 Q1 0101 - SG - African History and LiteratureДокумент13 страницME Eng 8 Q1 0101 - SG - African History and Literaturerosary bersanoОценок пока нет
- A Case Study Puga Geothermal System,: OF IndiaДокумент7 страницA Case Study Puga Geothermal System,: OF IndiaPERIKALA TARUNОценок пока нет
- Vendor Information Sheet - LFPR-F-002b Rev. 04Документ6 страницVendor Information Sheet - LFPR-F-002b Rev. 04Chelsea EsparagozaОценок пока нет
- Electives - ArchitДокумент36 страницElectives - Architkshitiz singhОценок пока нет
- 04 - Fetch Decode Execute Cycle PDFДокумент3 страницы04 - Fetch Decode Execute Cycle PDFShaun HaxaelОценок пока нет
- g6 - AFA - Q1 - Module 6 - Week 6 FOR TEACHERДокумент23 страницыg6 - AFA - Q1 - Module 6 - Week 6 FOR TEACHERPrincess Nicole LugtuОценок пока нет
- E0 UoE Unit 7Документ16 страницE0 UoE Unit 7Patrick GutierrezОценок пока нет
- User S Manual AURORA 1.2K - 2.2KДокумент288 страницUser S Manual AURORA 1.2K - 2.2KEprom ServisОценок пока нет
- Revenue and Expenditure AuditДокумент38 страницRevenue and Expenditure AuditPavitra MohanОценок пока нет
- DPSD ProjectДокумент30 страницDPSD ProjectSri NidhiОценок пока нет
- The Construction of Optimal Portfolio Using Sharpe's Single Index Model - An Empirical Study On Nifty Metal IndexДокумент9 страницThe Construction of Optimal Portfolio Using Sharpe's Single Index Model - An Empirical Study On Nifty Metal IndexRevanKumarBattuОценок пока нет
- Week 7Документ24 страницыWeek 7Priyank PatelОценок пока нет
- Farmer Producer Companies in OdishaДокумент34 страницыFarmer Producer Companies in OdishaSuraj GantayatОценок пока нет