Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlДокумент25 страницFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04Оценок пока нет
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Документ2 страницыIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04Оценок пока нет
- "Traditional" Exegeses of Q 4:34Документ15 страниц"Traditional" Exegeses of Q 4:34kiedd_04Оценок пока нет
- The Problems of Conscience and Hermeneutics: A Few Contemporary ApproachesДокумент15 страницThe Problems of Conscience and Hermeneutics: A Few Contemporary Approacheskiedd_04Оценок пока нет
- The Place For Others in IslamДокумент27 страницThe Place For Others in Islamkiedd_04Оценок пока нет
- In The Book We Have Left Out Nothing: The Ethical Problem of The Existence of Verse 4:34 in The QuranДокумент11 страницIn The Book We Have Left Out Nothing: The Ethical Problem of The Existence of Verse 4:34 in The Qurankiedd_04Оценок пока нет
- Blood (Part II)Документ68 страницBlood (Part II)kiedd_04100% (1)
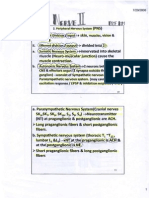
- Nerve Part IIДокумент5 страницNerve Part IIkiedd_04Оценок пока нет
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamДокумент13 страницOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- Synaptic Transmission ExercisesДокумент1 страницаSynaptic Transmission Exerciseskiedd_04Оценок пока нет
- Nerve Part IДокумент16 страницNerve Part Ikiedd_04Оценок пока нет
- Microbiology Colour Plate No.4Документ1 страницаMicrobiology Colour Plate No.4kiedd_04Оценок пока нет
- Matrix Table of Night Of Power (Arabic: لیلة القدر) 1430 Hijri, 2009Документ1 страницаMatrix Table of Night Of Power (Arabic: لیلة القدر) 1430 Hijri, 2009kiedd_04Оценок пока нет
- Nerve ExerciseДокумент2 страницыNerve Exercisekiedd_04Оценок пока нет
- Microbiology Colour Plate No.8Документ1 страницаMicrobiology Colour Plate No.8kiedd_04Оценок пока нет
- Cell PhysiologyДокумент61 страницаCell Physiologykiedd_04100% (4)
- Blood (Part I)Документ54 страницыBlood (Part I)kiedd_04Оценок пока нет
- Fadhilat Surah at TakwirДокумент1 страницаFadhilat Surah at Takwirkiedd_04Оценок пока нет
- Refleks ArcsДокумент34 страницыRefleks Arcskiedd_04100% (1)
- Introduction To PhysiologyДокумент38 страницIntroduction To Physiologykiedd_04Оценок пока нет
- Microbiology Colour Plate No.7Документ1 страницаMicrobiology Colour Plate No.7kiedd_04Оценок пока нет
- Microbiology Colour Plate No.6Документ1 страницаMicrobiology Colour Plate No.6kiedd_04Оценок пока нет
- Microbiology Colour Plate No.5Документ1 страницаMicrobiology Colour Plate No.5kiedd_04Оценок пока нет
- SYNAPSEДокумент35 страницSYNAPSEkiedd_04100% (3)
- Microbiology Colour Plate No.9Документ1 страницаMicrobiology Colour Plate No.9kiedd_04Оценок пока нет
- Microbiology Colour Plate No.2Документ1 страницаMicrobiology Colour Plate No.2kiedd_04Оценок пока нет
- Microbiology Colour Plate No.3Документ1 страницаMicrobiology Colour Plate No.3kiedd_04Оценок пока нет
- Bacteria Classification & Structure (MFEB 3402)Документ12 страницBacteria Classification & Structure (MFEB 3402)kiedd_04100% (1)
- Microbiology Colour Plate No.1Документ1 страницаMicrobiology Colour Plate No.1kiedd_04Оценок пока нет
- Vaccines (MFEB 3402)Документ17 страницVaccines (MFEB 3402)kiedd_04Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- EAU Pocket On Paediatric Urology 2023Документ54 страницыEAU Pocket On Paediatric Urology 2023Andrea SzaszОценок пока нет
- FimosisДокумент9 страницFimosiselsa relandaОценок пока нет
- Paediatric Urology - Peno-Scrotal: Case 1 Case 2Документ2 страницыPaediatric Urology - Peno-Scrotal: Case 1 Case 2HardiTariqHammaОценок пока нет
- CircumcisionДокумент19 страницCircumcisionKomite Medik RS Jiwa SofifiОценок пока нет
- BallooningДокумент4 страницыBallooningangginaharahapОценок пока нет
- Anomaly Genital in Children - RandyДокумент47 страницAnomaly Genital in Children - RandyAdhyatpОценок пока нет
- The PenisДокумент6 страницThe Penisntambik21Оценок пока нет
- PhimosisДокумент12 страницPhimosisSonia AnestesiaОценок пока нет
- Anomalies of The Penies ...Документ6 страницAnomalies of The Penies ...Firas Abu-SamraОценок пока нет
- Genital Surgical DiseasesДокумент18 страницGenital Surgical DiseasesanojОценок пока нет
- Definition of PhimosisДокумент11 страницDefinition of PhimosisAzizah Hafaz0% (1)
- Kontraindikasi CircumsisiДокумент23 страницыKontraindikasi CircumsisiElfi MuazzamОценок пока нет
- Obligatory Reading List:: Tasks That Students Must Complete in Order To Successfully Prepare For The Practical ClassДокумент4 страницыObligatory Reading List:: Tasks That Students Must Complete in Order To Successfully Prepare For The Practical ClassS VaibhavОценок пока нет
- Lection 8 SyphilisДокумент39 страницLection 8 SyphilisAtawna AtefОценок пока нет
- Paediatrics For Primary Care-01Документ31 страницаPaediatrics For Primary Care-01ZoranОценок пока нет
- Male Genital Representation in Palaeolithic ArtДокумент5 страницMale Genital Representation in Palaeolithic ArtcypmanОценок пока нет
- What Is Balanitis?Документ4 страницыWhat Is Balanitis?The OrthogirlОценок пока нет
- S1 Revision by Hania KhanДокумент87 страницS1 Revision by Hania KhanZoha AzizОценок пока нет
- Daftar Pustaka Fimosis ParafimosisДокумент1 страницаDaftar Pustaka Fimosis ParafimosisRuth Hanna KristianaОценок пока нет
- Review Article: Phimosis in ChildrenДокумент7 страницReview Article: Phimosis in ChildrenmerlinОценок пока нет
- Key Points: Information About Your Procedure From The British Association of Urological Surgeons (BAUS)Документ6 страницKey Points: Information About Your Procedure From The British Association of Urological Surgeons (BAUS)diva aurelliaОценок пока нет
- Kelainan Penis Pada AnakДокумент23 страницыKelainan Penis Pada AnakAndrew SoerijadiОценок пока нет
- Carcinoma of Penis: DR Hitesh Patel Associate Professor Surgery Department GMERS Medical College, GotriДокумент55 страницCarcinoma of Penis: DR Hitesh Patel Associate Professor Surgery Department GMERS Medical College, Gotrihitesh3150% (1)
- Era University / Era College of Nursing: Lesson Plan On-Congenital MalformationsДокумент14 страницEra University / Era College of Nursing: Lesson Plan On-Congenital MalformationsShreya Sinha100% (1)
- K25 - A - Congenital Anomalies of The Urinary TractДокумент26 страницK25 - A - Congenital Anomalies of The Urinary TractErwin SiregarОценок пока нет
- Standard Treatment Guidelines General Surgery: Ministry of Health & Family Welfare Govt. of IndiaДокумент73 страницыStandard Treatment Guidelines General Surgery: Ministry of Health & Family Welfare Govt. of IndiaiuytrerОценок пока нет
- Indication, Contraindication and Complication of CircumcisionДокумент16 страницIndication, Contraindication and Complication of CircumcisionRd manОценок пока нет
- The Causes and Treatment of BalanitisДокумент5 страницThe Causes and Treatment of BalanitisHugo RanziОценок пока нет
- GFP EnauДокумент2 страницыGFP EnauDomenico BevilacquaОценок пока нет
- CNCM 229 Reproductive DisordersДокумент12 страницCNCM 229 Reproductive DisordersRaven Renz OngОценок пока нет