Вам также может понравиться
- Posture in PhysiotherapyДокумент31 страницаPosture in PhysiotherapyAnshuman VyasОценок пока нет
- Posture PDFДокумент30 страницPosture PDFSairelle Sordilla Obang100% (1)
- Posture AnalysisДокумент45 страницPosture AnalysisPriyanka Choursiya100% (1)
- Theme 3. Lumbopelvic Motor Control, Instability and PainДокумент9 страницTheme 3. Lumbopelvic Motor Control, Instability and PainThéo BattalianОценок пока нет
- PostureДокумент72 страницыPosture69016100% (1)
- Posture Dr. Dr. MY, SP KFR-KДокумент67 страницPosture Dr. Dr. MY, SP KFR-KCikupaОценок пока нет
- Retdem ModДокумент3 страницыRetdem ModHanna BuadaОценок пока нет
- Therapeutic Postuure 2020 1,2,3Документ116 страницTherapeutic Postuure 2020 1,2,3Mustafa Mabrouk100% (2)
- PostureДокумент20 страницPostureAnita Gajari100% (2)
- Biomechanics of Posture PDFДокумент20 страницBiomechanics of Posture PDFPhooi Yee Lau89% (9)
- Joint Mobilization What Is Joint Mobilization?Документ6 страницJoint Mobilization What Is Joint Mobilization?taravindnagarajОценок пока нет
- Article Perfect Posture PuzzleДокумент6 страницArticle Perfect Posture PuzzleMuhammad FahmyОценок пока нет
- Chap 14-1Документ29 страницChap 14-1abdul hannanОценок пока нет
- Rehabilitation and Treatments of Sports InjuriesДокумент20 страницRehabilitation and Treatments of Sports InjuriesRAJESH MALIKОценок пока нет
- Joint Mobilization ExercisesДокумент19 страницJoint Mobilization ExercisesManju ElangovanОценок пока нет
- Biomechanics of The Spine1 (Chapter5.t)Документ24 страницыBiomechanics of The Spine1 (Chapter5.t)Z .TОценок пока нет
- Movement Posture and AlignmentДокумент6 страницMovement Posture and AlignmentShivalikaОценок пока нет
- Posture Project 1 FinalДокумент79 страницPosture Project 1 FinalASHU KОценок пока нет
- Exploring Perfect PostureДокумент8 страницExploring Perfect Posturesquishyware100% (1)
- Somatic Anatomy Muscles and The Postural FluteДокумент6 страницSomatic Anatomy Muscles and The Postural FlutearonolamОценок пока нет
- CogwheelДокумент4 страницыCogwheelRimsha RanaОценок пока нет
- Core StabilityДокумент3 страницыCore StabilityGonzalo GonzalesОценок пока нет
- Core StabilityДокумент3 страницыCore StabilityGonzalo GonzalesОценок пока нет
- PostureДокумент20 страницPostureBalram Jha100% (1)
- CHP 11Документ71 страницаCHP 11Sophia YounОценок пока нет
- PT3 Postural AnalysisДокумент5 страницPT3 Postural Analysisim. EliasОценок пока нет
- Posture: Deswaty Furqonita, Ssi, MbiomedДокумент30 страницPosture: Deswaty Furqonita, Ssi, MbiomedYusuf HidayatОценок пока нет
- Effect of Core Stabilization Training On Endurance of Trunk Extensor and Functional Capacity in Subjects With Mechanical Low Back PainДокумент8 страницEffect of Core Stabilization Training On Endurance of Trunk Extensor and Functional Capacity in Subjects With Mechanical Low Back PainDr. Krishna N. SharmaОценок пока нет
- Muscular System NotesДокумент40 страницMuscular System NotesWindhy Dzakiyyah Aurora100% (1)
- 11 Muscularfitness 5d8c6a01254ddДокумент39 страниц11 Muscularfitness 5d8c6a01254ddZahra AdzkiaОценок пока нет
- Manual MCQZДокумент9 страницManual MCQZFarah IqbalОценок пока нет
- Musculoskeletal Assessment: Structures of The MS SystemДокумент10 страницMusculoskeletal Assessment: Structures of The MS SystemSherwin B. CaytapОценок пока нет
- Topic:-Posture: Dr:Maryam Memon Lecturer: JmiprsДокумент43 страницыTopic:-Posture: Dr:Maryam Memon Lecturer: JmiprsAazeen memonОценок пока нет
- Trios: Key Terms: Center of GravityДокумент45 страницTrios: Key Terms: Center of GravityStefanie Kiss-PlucasОценок пока нет
- PostureДокумент24 страницыPostureBhargavОценок пока нет
- 1 Degrees of Freedom: Rigid Body FixityДокумент2 страницы1 Degrees of Freedom: Rigid Body FixityCarl SorensenОценок пока нет
- Normal End Feel Abnormal End Feel: ST NDДокумент2 страницыNormal End Feel Abnormal End Feel: ST NDsungmin kimОценок пока нет
- Aarti - Introduction of Biomechanics PostureДокумент64 страницыAarti - Introduction of Biomechanics PostureKalyani Savant0% (1)
- The Effects of Serial Stretch Loading On Stretch Work and Stretch-Shorten Cycle Performance in The Knee MusculatureДокумент11 страницThe Effects of Serial Stretch Loading On Stretch Work and Stretch-Shorten Cycle Performance in The Knee MusculatureraomanishОценок пока нет
- Lec#1 Basic TerminologiesДокумент42 страницыLec#1 Basic TerminologiesUsman FarooqОценок пока нет
- Balance Training and Exercise in Geriatric Patients: M. Runge, G. Rehfeld, E. ResnicekДокумент6 страницBalance Training and Exercise in Geriatric Patients: M. Runge, G. Rehfeld, E. ResnicekVicky LumalessilОценок пока нет
- PDF CrackДокумент12 страницPDF Crackdj_reaverОценок пока нет
- 1 Human PostureДокумент21 страница1 Human PostureLeiОценок пока нет
- Fundamentals FinalsДокумент24 страницыFundamentals FinalserythromycinОценок пока нет
- The Posture & Righting Reflexes (Guyton Ed. 13: Pg. 704-705)Документ21 страницаThe Posture & Righting Reflexes (Guyton Ed. 13: Pg. 704-705)Mudassar SattarОценок пока нет
- Yogic Management of BackPainДокумент29 страницYogic Management of BackPainJacklynlim LkcОценок пока нет
- Mobility Activity Positioning Massage PainДокумент20 страницMobility Activity Positioning Massage Pain황춘히Оценок пока нет
- Dossier RPG EnglishДокумент15 страницDossier RPG EnglishtetevoОценок пока нет
- Hamstrings - Mechanics, Injury and Rehabilitation. Christopher NorrisДокумент9 страницHamstrings - Mechanics, Injury and Rehabilitation. Christopher NorrisPascu MariusОценок пока нет
- THIRD, Any Rebound Contact Force From TheДокумент10 страницTHIRD, Any Rebound Contact Force From TheKcaBbe JavierОценок пока нет
- Introduction To Exercise TherapyДокумент29 страницIntroduction To Exercise TherapyAhmed100% (3)
- ACE Personal Trainer Manual, 4 Edition: Functional Programming For Stability-Mobility and MovementДокумент94 страницыACE Personal Trainer Manual, 4 Edition: Functional Programming For Stability-Mobility and MovementManjunatha GayakwadОценок пока нет
- Muscular ConsiderationsДокумент59 страницMuscular ConsiderationsThor ManlangitОценок пока нет
- The Features of Bones and Joints: Sanae Silvera 11j Shannay Mckenzie 11jДокумент10 страницThe Features of Bones and Joints: Sanae Silvera 11j Shannay Mckenzie 11jshannay mckenzieОценок пока нет
- Modeling of The Musculoskeletal System - 1Документ9 страницModeling of The Musculoskeletal System - 1Shyam PolacondaОценок пока нет
- Ortho Assessment PDFДокумент9 страницOrtho Assessment PDFtafelaОценок пока нет
- Burns and The Physiotherapist: Royal Melbourne HospitalДокумент5 страницBurns and The Physiotherapist: Royal Melbourne HospitalBennat RajОценок пока нет
- Physiotherapyintheintensivecareunit: ReviewДокумент10 страницPhysiotherapyintheintensivecareunit: ReviewBennat RajОценок пока нет
- Para Medical Courses - 2020 - 2021 Session List of Candidates Allotted On 09.02.2021Документ9 страницPara Medical Courses - 2020 - 2021 Session List of Candidates Allotted On 09.02.2021Bennat RajОценок пока нет
- Rehabilitation of Neurogenic Bladder Function Workshop 22 Monday 23 August 2010, 14:00 - 18:00Документ25 страницRehabilitation of Neurogenic Bladder Function Workshop 22 Monday 23 August 2010, 14:00 - 18:00Bennat RajОценок пока нет
- A Field Comparison of Neck and Shoulder Postures in Symptomatic and Asymptomatic o Ce WorkersДокумент10 страницA Field Comparison of Neck and Shoulder Postures in Symptomatic and Asymptomatic o Ce WorkersBennat RajОценок пока нет
- The Active Cycle of Breathing Techniques: Oxford University HospitalsДокумент8 страницThe Active Cycle of Breathing Techniques: Oxford University HospitalsBennat RajОценок пока нет
- Para Medical Courses - 2019 - 2020 Session List of Candidates Allotted On 10.09.2019Документ97 страницPara Medical Courses - 2019 - 2020 Session List of Candidates Allotted On 10.09.2019Bennat RajОценок пока нет
- Stroke 2 RCTДокумент6 страницStroke 2 RCTArdhyan ArdhyanОценок пока нет
- Relationshipposturealcontrol FMAJOTNovember 2011Документ8 страницRelationshipposturealcontrol FMAJOTNovember 2011Bennat RajОценок пока нет
- A Practical Physiotherapy Approach in Intensive Care UnitДокумент11 страницA Practical Physiotherapy Approach in Intensive Care UnitBennat RajОценок пока нет
- Electric Muscle Stimulation of The Quadriceps in The Treatment of Patellofemoral PainДокумент7 страницElectric Muscle Stimulation of The Quadriceps in The Treatment of Patellofemoral PainBennat RajОценок пока нет
- Allied Sciences (Cbe Colleges) Fees 2020-21Документ4 страницыAllied Sciences (Cbe Colleges) Fees 2020-21Bennat RajОценок пока нет
- Why and How Are Posture and Movement Coordinated?: Progress in Brain Research February 2004Документ16 страницWhy and How Are Posture and Movement Coordinated?: Progress in Brain Research February 2004BogdanОценок пока нет
- NCERT Class 12 BiologyДокумент311 страницNCERT Class 12 Biologynaveen reddy100% (1)
- PDF DocumentДокумент151 страницаPDF DocumentBennat RajОценок пока нет
- The Effects of Sitting Questionmark Exercise and Brugger's Relief Exercise On Pain, ROM, Proprioception, NDI in Patients With Chronic Cervical PainДокумент9 страницThe Effects of Sitting Questionmark Exercise and Brugger's Relief Exercise On Pain, ROM, Proprioception, NDI in Patients With Chronic Cervical PainBennat RajОценок пока нет
- Validity and Reliability of Shyam 360 Posture Grid: A Tool For The Assessment of Human PostureДокумент4 страницыValidity and Reliability of Shyam 360 Posture Grid: A Tool For The Assessment of Human PostureBennat RajОценок пока нет
- Methods of Postural Assessment Used For Sports Persons: Abst TДокумент4 страницыMethods of Postural Assessment Used For Sports Persons: Abst TUmesh BhandariОценок пока нет
- Validity and Reliability of Shyam 360 Posture Grid: A Tool For The Assessment of Human PostureДокумент4 страницыValidity and Reliability of Shyam 360 Posture Grid: A Tool For The Assessment of Human PostureBennat RajОценок пока нет
- Physiotherapy For Anterior Knee Pain: A Randomised Controlled TrialДокумент5 страницPhysiotherapy For Anterior Knee Pain: A Randomised Controlled TrialBennat RajОценок пока нет
- Training Program and Additional Electric Muscle Stimulation For Patellofemoral Pain Syndrome: A Pilot StudyДокумент7 страницTraining Program and Additional Electric Muscle Stimulation For Patellofemoral Pain Syndrome: A Pilot StudyBennat RajОценок пока нет
- Mid-Thoracic Dysfunction: A Key Perpetuating Factor of Pain in The Locomotor SystemДокумент5 страницMid-Thoracic Dysfunction: A Key Perpetuating Factor of Pain in The Locomotor SystemBennat RajОценок пока нет
- Validity and Reliability of Shyam 360 Posture Grid: A Tool For The Assessment of Human PostureДокумент4 страницыValidity and Reliability of Shyam 360 Posture Grid: A Tool For The Assessment of Human PostureBennat RajОценок пока нет
- Effect of Mckenzie Self-Therapy Protocol On Forward Head Posture and Respiratory Functions of School Going Adolescent GirlsДокумент6 страницEffect of Mckenzie Self-Therapy Protocol On Forward Head Posture and Respiratory Functions of School Going Adolescent GirlsBennat RajОценок пока нет
- Self Help Advice For The Clinician SelfДокумент9 страницSelf Help Advice For The Clinician SelfBennat RajОценок пока нет
- Section 2:: Clinical UpdateДокумент2 страницыSection 2:: Clinical UpdateBennat RajОценок пока нет
- MM SS Bruggers Seated StretchДокумент1 страницаMM SS Bruggers Seated StretchFernandoОценок пока нет
- Self Treatment of Mid Thoracic Dysfunction - A Key Link in The Body Axis Part 1Документ9 страницSelf Treatment of Mid Thoracic Dysfunction - A Key Link in The Body Axis Part 1Bennat RajОценок пока нет
- Project in BiologyДокумент5 страницProject in BiologyViah TronzalОценок пока нет
- Journey Into The World of Biology CellsДокумент8 страницJourney Into The World of Biology CellsNazar MuhammadОценок пока нет
- Lab Manual 11102016 PDFДокумент239 страницLab Manual 11102016 PDFDesyAyu DzulfaAry EomutОценок пока нет
- Renal OsteodistrophyДокумент18 страницRenal OsteodistrophyFadlan ADima AdriantaОценок пока нет
- HydrocephalusДокумент40 страницHydrocephalusAstrid Sabirin100% (1)
- Molecular Genetics of Endometrial CancerДокумент31 страницаMolecular Genetics of Endometrial CancerJoju SebastianОценок пока нет
- Metastatic Vertebral Lesion Mimicking An Atypical Hemangioma WithДокумент8 страницMetastatic Vertebral Lesion Mimicking An Atypical Hemangioma Withsica_17_steaua6519Оценок пока нет
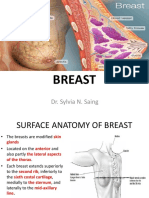
- Breast: Dr. Sylvia N. SaingДокумент26 страницBreast: Dr. Sylvia N. SaingRichard 151289100% (1)
- Medical NotesДокумент421 страницаMedical NotesDanielle100% (7)
- Mrcs Part B StationsДокумент2 страницыMrcs Part B Stationsprashanth naikОценок пока нет
- APCH1 - Single Chain Antibody For Vaccine TargetingДокумент6 страницAPCH1 - Single Chain Antibody For Vaccine TargetingAgustín OstachukОценок пока нет
- Blood Cell Morphology TutorialДокумент176 страницBlood Cell Morphology TutorialCharles Jebb Belonio JuanitasОценок пока нет
- World of PlantsДокумент3 страницыWorld of PlantsWinter Summer SmithОценок пока нет
- Pharmaceutical Sciences: ArticleinfoДокумент8 страницPharmaceutical Sciences: ArticleinfoMario CastroОценок пока нет
- Skeletal SystemДокумент1 страницаSkeletal SystemEzekiel De GuzmanОценок пока нет
- Aristotle S Anatomical Philosophy of NatureДокумент29 страницAristotle S Anatomical Philosophy of NatureManuel AvataresОценок пока нет
- Jove-84-51214 - Vasectomy, Mouse ModelДокумент8 страницJove-84-51214 - Vasectomy, Mouse ModelGia KuteliaОценок пока нет
- Holiday Package Biology f4 2017Документ2 страницыHoliday Package Biology f4 2017putri_latifahОценок пока нет
- Assisting A Normal Spontaneous Delivery ChecklistДокумент3 страницыAssisting A Normal Spontaneous Delivery ChecklistPia CastilloОценок пока нет
- 6th Class Digestive SystemДокумент20 страниц6th Class Digestive SystemJuvy MarquinezОценок пока нет
- Giant Omphalocele With OEIS Complex - A Case ReportДокумент3 страницыGiant Omphalocele With OEIS Complex - A Case ReportIOSRjournalОценок пока нет
- 9.intracellular Accumulations 1Документ45 страниц9.intracellular Accumulations 1Ramesh KumarОценок пока нет
- CBSE Class X Biology - Life Processs Key NotesДокумент18 страницCBSE Class X Biology - Life Processs Key NotesBhavesh DesaiОценок пока нет
- Red Blood CellsДокумент2 страницыRed Blood CellsArina FarahdibaОценок пока нет
- Histology of Male Reproductive SystemДокумент56 страницHistology of Male Reproductive SystemMuhammad Irfan100% (2)
- CARDIOVASCULAR ANATOMY AND PHYSIOLOGY TestДокумент6 страницCARDIOVASCULAR ANATOMY AND PHYSIOLOGY TestDevilsnareОценок пока нет
- Case Study of A Patient With Ischemic CardiomyopathyДокумент33 страницыCase Study of A Patient With Ischemic Cardiomyopathyromeo rivera80% (5)
- How To Do Lymphatic Self-Massage On Your Face, Head and NeckДокумент11 страницHow To Do Lymphatic Self-Massage On Your Face, Head and NeckGleda SaavedraОценок пока нет
- Chapter 2 - Anatomy Posture and Body MechanicsДокумент53 страницыChapter 2 - Anatomy Posture and Body MechanicsRogini Sindhu100% (6)
- Endocrine System-Worksheet MTIДокумент4 страницыEndocrine System-Worksheet MTIKolynОценок пока нет