Please Complete ALL Blanks
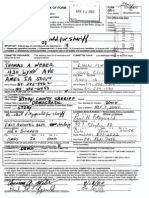
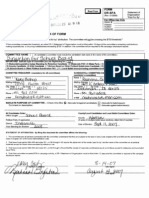
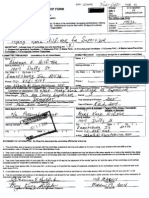
FORM I
STATE"
Check One : ORGANIZATION
O
CANDIDATE
o This is an Initial' Statement of Organization
For office use gall
This is an Amended' Statement of Organization
'A new Statement of Organization should be filed within 10 days of l c rp i s tributions, Comm. # 17304
making expenditures or incurring indebtedness exceeding $500 i a calendar year. Amendments should Indexed
be filed within 30 days of a change . Audited
Checked
STORY COU - I - AUDITOR
Computer
CANDIDATE COMMITTEE NAME
Official Name of Candidate Comrgitt-e (Identify acronyms. Last name of candidate shoWd be part of official name.)
T-F-tit-gcT HALL16UtToN CGMM1'TT6E
Mailing Address of committee if a separate headquarters is established.
II& P-665EYecr
City State Zip Code Area Code Telephone
A+M E 5 ~4 .54010 -5"97 4 515- -
COMMITTEE TREASURER (Must bean Iowa resident of ma)odly age.) COMMITTEE CHAIR (Ustotherofficers asnquired bylaw ff-)
Name
NFk'ANKL11V J . FEII MEYEk,
Maili Address (T^
his address used for all reminders and correspondence) Mailing Address
1 t 9 Gie-Aryb AvE-
p Code Area
Telephone City . State- Zip Code Area Telephone
AMES 50010 Code
t
FINANCIAL INSTITUTION IN WHICH FUNDS ARE DEPOSITED (MUST BE LOCATED IN IOWA)
Candidate Committees are required by law to deposit all funds and pay all bills from a separate account, and to disclose the name of the financial Institution
where funds are deposited. Use back of form if more than one. Exception: If all campaign expenses will be paid from personal funds and no donations
will be accepted, separate account not required.
Name of Financial Institution (Bank, Savings & Loan. Credit Union, etc)
FIRST ///47-/OA//9,4- q-K4
Mailing Address Name of account as shown on checks and bank statement
I ;~
y FF
lJ2 ~clETT T F'' EC . EcT ~f}LL r~U,eT6K ~G/~fM! TTEF
City Zip Code Type of Account (checking, swings, certificate of deposit, etc.)
AME5 .J'Q-
-J-'Q ~QO/0 CNECK11 l
CANDIDATE SUPPORTED
Name of Candidate ~~ /~
5
Office Sought county
JA N F. E. t1 ALL 1,6 01.To lJ t- 0unl-T Y U GE4 V 1501Z , 5TO/
Address (Home)~ Political Party (Democrat Republican, Independent, etc. Year Standing for Election
X. 00 5 ~--= VEL7- --J)EAJ 0 C C R7 - l 9 9~
City State Zip Code Arm Code Telephone
At~s --rn . 5o6l0 515 - l
DISPOSITION OF BALANCE OF FUNDS UPON DISSOLUTION
All candidates are required to make a statement of intent of how leftover funds would be expended at the close of the campaign when
the committee is dissolved. This statement may be amended at a later date if the candidate chooses. The statement must be made,
even if the candidate anticipates there will be no leftover funds . The choices listed below are the ONLY legal options in accordance
with Iowa Code 56 .42 .
CHECK ONE AND ENTER SPECIFIC NAME :
13 Return Prorata to Contributors
0 Donate to Local Political Party
13 Transfer to State of Iowa General Fund
V Donate to 57'OO2 i County Central Committee
E3 Transfer to Charitable Organization -
13 Donate to State Political Party
0 Donate to National Political Party (Specify Charitable Organization)
0 Transfer to another committe of this same candidate
STATEMENT OF AFFIRMATION BY TREASURER AND CANDIDATE
I am aware that disclosure reports are required if the committee and/or candidate receives contributions, makes expenditures, or incurs
indebtedness in excess of five hundred dollars in a calendar year for the purpose of supporting or opposing any candidate for public office.
1 am also aware that late filed reports are subject to civil penalties (fines) under the disclosure law. I also understand that although the
res and files reports, the candidate is responsible under the law for accurate and timely disclosure reports.
nature of Treasurer Date Signed
I
/99
Signature
of Candidate Date Signed
ttPK-02051140-0063(N)/(Rev . 199C;)
Вам также может понравиться
- Internship Report On Soneri Bank LimitedДокумент78 страницInternship Report On Soneri Bank LimitedZubair Khan50% (2)
- August 2021Документ1 страницаAugust 2021Julio DelarozaОценок пока нет
- A o ' ST: For Instructions, See Back of FormДокумент1 страницаA o ' ST: For Instructions, See Back of FormZach EdwardsОценок пока нет
- For Instructions, See Back of Form Check One: This Is LДокумент1 страницаFor Instructions, See Back of Form Check One: This Is LZach EdwardsОценок пока нет
- 2005 09 06 DR1Документ2 страницы2005 09 06 DR1Zach EdwardsОценок пока нет
- 2004 12 08 - DR1Документ1 страница2004 12 08 - DR1Zach EdwardsОценок пока нет
- 2004-08-24 DR1 AmendedДокумент1 страница2004-08-24 DR1 AmendedZach EdwardsОценок пока нет
- 2005 01 17 - DR1Документ1 страница2005 01 17 - DR1Zach EdwardsОценок пока нет
- 2002 09 03 - DR1Документ1 страница2002 09 03 - DR1Zach EdwardsОценок пока нет
- 2004-11-24 DR1 AmendedДокумент1 страница2004-11-24 DR1 AmendedZach EdwardsОценок пока нет
- 2000 04 24 - DR1Документ1 страница2000 04 24 - DR1Zach EdwardsОценок пока нет
- 2006-05-26 SfaДокумент1 страница2006-05-26 SfaZach EdwardsОценок пока нет
- 1992 03 12 - DR1Документ1 страница1992 03 12 - DR1Zach EdwardsОценок пока нет
- 2002 09 18 - DR1Документ1 страница2002 09 18 - DR1Zach EdwardsОценок пока нет
- 2005-11-04 DR1Документ1 страница2005-11-04 DR1Zach EdwardsОценок пока нет
- For Instructions, See Back of Form DR-1: REC ®ived SEP 18 2007Документ1 страницаFor Instructions, See Back of Form DR-1: REC ®ived SEP 18 2007Zach EdwardsОценок пока нет
- For Instructions, See Back of Form Camp '' An I3Isgluo FW CK One: OF . . DRA IsДокумент1 страницаFor Instructions, See Back of Form Camp '' An I3Isgluo FW CK One: OF . . DRA IsZach EdwardsОценок пока нет
- I5 E06LON A'Je: For Instructions, See Back of Form 0Документ17 страницI5 E06LON A'Je: For Instructions, See Back of Form 0Zach EdwardsОценок пока нет
- Wilhelm, Mary Jo 1717Документ1 страницаWilhelm, Mary Jo 1717Zach EdwardsОценок пока нет
- For Instructions, See Back of Fo4 Form DR-1Документ1 страницаFor Instructions, See Back of Fo4 Form DR-1Zach EdwardsОценок пока нет
- Notice of Dissolution: Mail To: Iecdi3 510 East 12'h, Suite IA Des Moines, Iowa 50319 I Reset Form DR-3Документ5 страницNotice of Dissolution: Mail To: Iecdi3 510 East 12'h, Suite IA Des Moines, Iowa 50319 I Reset Form DR-3Zach EdwardsОценок пока нет
- 2004 10 21 - DR1Документ1 страница2004 10 21 - DR1Zach EdwardsОценок пока нет
- For Instructions, See Back of Form DR-1: M-Ciiia-A. 505-ZДокумент1 страницаFor Instructions, See Back of Form DR-1: M-Ciiia-A. 505-ZZach EdwardsОценок пока нет
- 2007-08-29 Dr-SfaДокумент1 страница2007-08-29 Dr-SfaZach EdwardsОценок пока нет
- Kramer 10 19 05Документ1 страницаKramer 10 19 05Zach EdwardsОценок пока нет
- 2004 02 13 - DR1Документ1 страница2004 02 13 - DR1Zach EdwardsОценок пока нет
- Ikt Is +: For Instructions, See Back of Form Dr-1Документ1 страницаIkt Is +: For Instructions, See Back of Form Dr-1Zach EdwardsОценок пока нет
- M, 1re T tJE C, 4: For Instructions, See Back of Form Check OneДокумент3 страницыM, 1re T tJE C, 4: For Instructions, See Back of Form Check OneZach EdwardsОценок пока нет
- 2005 09 28 - DR1Документ1 страница2005 09 28 - DR1Zach EdwardsОценок пока нет
- 2006 01 26 - DR1Документ1 страница2006 01 26 - DR1Zach EdwardsОценок пока нет
- 2006-07-20 DR1 AmendmentДокумент1 страница2006-07-20 DR1 AmendmentZach EdwardsОценок пока нет
- 2001 10 11 - DR1Документ1 страница2001 10 11 - DR1Zach EdwardsОценок пока нет
- 2005 10 20 - DR1Документ1 страница2005 10 20 - DR1Zach EdwardsОценок пока нет
- Qwest 10 14 05Документ1 страницаQwest 10 14 05Zach EdwardsОценок пока нет
- Receive: For Instructions, See Back of Form Form DR-1Документ1 страницаReceive: For Instructions, See Back of Form Form DR-1Zach EdwardsОценок пока нет
- For Instructions, See Back of Form Form DR-1: Committee Name 1 1Документ1 страницаFor Instructions, See Back of Form Form DR-1: Committee Name 1 1Zach EdwardsОценок пока нет
- Eaton, Josh 1712Документ1 страницаEaton, Josh 1712Zach EdwardsОценок пока нет
- For Instructions, See Back of Form DR-1Документ1 страницаFor Instructions, See Back of Form DR-1Zach EdwardsОценок пока нет
- 2006 04 19 - DR1Документ1 страница2006 04 19 - DR1Zach EdwardsОценок пока нет
- 2004 10 18 - DR1Документ1 страница2004 10 18 - DR1Zach EdwardsОценок пока нет
- For Instructions, See Back of F Chfiick One: L RM Dr-1: Committee Name 1Документ1 страницаFor Instructions, See Back of F Chfiick One: L RM Dr-1: Committee Name 1Zach EdwardsОценок пока нет
- 2005 08 01 - DR1Документ1 страница2005 08 01 - DR1Zach EdwardsОценок пока нет
- 2005 11 01 - DR1Документ1 страница2005 11 01 - DR1Zach EdwardsОценок пока нет
- 2005 10 08 - DR1Документ2 страницы2005 10 08 - DR1Zach EdwardsОценок пока нет
- Iixml D, - 1: - or Instructions, See Back of Form Ieck One: Initial"' Amended''Документ1 страницаIixml D, - 1: - or Instructions, See Back of Form Ieck One: Initial"' Amended''Zach EdwardsОценок пока нет
- 2006 03 16 - DR1Документ1 страница2006 03 16 - DR1Zach EdwardsОценок пока нет
- Qwest 10 19 05Документ1 страницаQwest 10 19 05Zach EdwardsОценок пока нет
- Knupp For Mayor: For Instructions, See Back of Form LДокумент1 страницаKnupp For Mayor: For Instructions, See Back of Form LZach EdwardsОценок пока нет
- For Instructions, See Back of Form: Acoap Mupt W DamДокумент1 страницаFor Instructions, See Back of Form: Acoap Mupt W DamZach EdwardsОценок пока нет
- For Instructions, See Back of Form: For Office Use OnlyДокумент1 страницаFor Instructions, See Back of Form: For Office Use OnlyZach EdwardsОценок пока нет
- 2005 05 02 - DR1Документ1 страница2005 05 02 - DR1Zach EdwardsОценок пока нет
- For Instructions, See Back of Form Check O: An Initial" Statement of His Is An Amended" Statement of C RLTRB o S. S oДокумент1 страницаFor Instructions, See Back of Form Check O: An Initial" Statement of His Is An Amended" Statement of C RLTRB o S. S oZach EdwardsОценок пока нет
- Melanie Bates 09 01 05Документ1 страницаMelanie Bates 09 01 05Zach EdwardsОценок пока нет
- Instructions, See Back of For CK One: DR-1 OF: This Is Initial This Is Amended" Reset - Form For OfficeДокумент1 страницаInstructions, See Back of For CK One: DR-1 OF: This Is Initial This Is Amended" Reset - Form For OfficeZach EdwardsОценок пока нет
- 2006 11 22 - DR1Документ1 страница2006 11 22 - DR1Zach EdwardsОценок пока нет
- 2005 09 16 - DR1Документ1 страница2005 09 16 - DR1Zach EdwardsОценок пока нет
- V%Oulnth: For Instructions, See Back of Form I Ugi L U Form Dr-1Документ2 страницыV%Oulnth: For Instructions, See Back of Form I Ugi L U Form Dr-1Zach EdwardsОценок пока нет
- For Instructions, See Back of Form 0 Dr-1: '-L' (Aec Jaisg-WenueДокумент1 страницаFor Instructions, See Back of Form 0 Dr-1: '-L' (Aec Jaisg-WenueZach EdwardsОценок пока нет
- For Instructions - See Sack of Form DR-1Документ1 страницаFor Instructions - See Sack of Form DR-1Zach EdwardsОценок пока нет
- 2005 07 18 - DR1Документ1 страница2005 07 18 - DR1Zach EdwardsОценок пока нет
- For Instructions, See Back of Form Check One:: MarungДокумент1 страницаFor Instructions, See Back of Form Check One:: MarungZach EdwardsОценок пока нет
- Third Quarterly ReportДокумент3 страницыThird Quarterly ReportZach EdwardsОценок пока нет
- PACEG Committee (Political Action Comm. For Effect. Govt) - 6112 - EДокумент1 страницаPACEG Committee (Political Action Comm. For Effect. Govt) - 6112 - EZach EdwardsОценок пока нет
- Second Quarterly ReportДокумент3 страницыSecond Quarterly ReportZach EdwardsОценок пока нет
- Year-End ReportДокумент12 страницYear-End ReportZach EdwardsОценок пока нет
- PACEG Committee (Political Action Comm. For Effect. Govt) - 6112 - EДокумент1 страницаPACEG Committee (Political Action Comm. For Effect. Govt) - 6112 - EZach EdwardsОценок пока нет
- Olson, Steve - Steve Olson For State Representative - 1387 - A - ContributionsДокумент2 страницыOlson, Steve - Steve Olson For State Representative - 1387 - A - ContributionsZach EdwardsОценок пока нет
- Second Quarterly ReportДокумент3 страницыSecond Quarterly ReportZach EdwardsОценок пока нет
- Third Quarterly ReportДокумент3 страницыThird Quarterly ReportZach EdwardsОценок пока нет
- Third Quarterly ReportДокумент3 страницыThird Quarterly ReportZach EdwardsОценок пока нет
- Olson, Rick - Committee To Elect Rick Olson To House of Representatives - 1560 - DR1Документ2 страницыOlson, Rick - Committee To Elect Rick Olson To House of Representatives - 1560 - DR1Zach EdwardsОценок пока нет
- Olson, Steve - Steve Olson For State Representative - 1387 - DR1Документ2 страницыOlson, Steve - Steve Olson For State Representative - 1387 - DR1Zach EdwardsОценок пока нет
- Iowa Laborers Political Action Committee - 6449 - B - ExpendituresДокумент3 страницыIowa Laborers Political Action Committee - 6449 - B - ExpendituresZach EdwardsОценок пока нет
- Olson, Steve - Steve Olson For State Representative - 1387 - DR2 - SummaryДокумент1 страницаOlson, Steve - Steve Olson For State Representative - 1387 - DR2 - SummaryZach EdwardsОценок пока нет
- Olson, Steve - Steve Olson For State Representative - 1387 - B - ExpendituresДокумент1 страницаOlson, Steve - Steve Olson For State Representative - 1387 - B - ExpendituresZach EdwardsОценок пока нет
- Olson, Rick - Committee To Elect Rick Olson To House of Representatives - 1560 - DR1Документ2 страницыOlson, Rick - Committee To Elect Rick Olson To House of Representatives - 1560 - DR1Zach EdwardsОценок пока нет
- Wipperman, Citizens For Wipperman - 1670 - DR2 - SummaryДокумент1 страницаWipperman, Citizens For Wipperman - 1670 - DR2 - SummaryZach EdwardsОценок пока нет
- Olson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - DR2 - SummaryДокумент1 страницаOlson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - DR2 - SummaryZach EdwardsОценок пока нет
- Wipperman, Citizens For Wipperman - 1670 - DR2 - SummaryДокумент1 страницаWipperman, Citizens For Wipperman - 1670 - DR2 - SummaryZach EdwardsОценок пока нет
- Olson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - DR1Документ2 страницыOlson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - DR1Zach EdwardsОценок пока нет
- Olson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - E - in - KindДокумент1 страницаOlson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - E - in - KindZach EdwardsОценок пока нет
- Olson, Olson For State Representative Committee, Donovan Olson, Can - 1392 - A - ContributionsДокумент9 страницOlson, Olson For State Representative Committee, Donovan Olson, Can - 1392 - A - ContributionsZach EdwardsОценок пока нет
- Reynolds, Committee To Re-Elect Representative Reynolds - 1052 - BДокумент1 страницаReynolds, Committee To Re-Elect Representative Reynolds - 1052 - BZach EdwardsОценок пока нет
- Olson, Olson For State Representative Committee, Donovan Olson, Can - 1392 - AДокумент7 страницOlson, Olson For State Representative Committee, Donovan Olson, Can - 1392 - AZach EdwardsОценок пока нет
- Olson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - DR1Документ2 страницыOlson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - DR1Zach EdwardsОценок пока нет
- Olson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - A - ContributionsДокумент1 страницаOlson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - A - ContributionsZach EdwardsОценок пока нет
- Olson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - B - ExpendituresДокумент1 страницаOlson, Donovan - Olson For State Representative Committee, Donovan Olson, Can - 1392 - B - ExpendituresZach EdwardsОценок пока нет
- Olson, Dennis - Dennis Olson For Representative - 1920 - DR2 - SummaryДокумент1 страницаOlson, Dennis - Dennis Olson For Representative - 1920 - DR2 - SummaryZach EdwardsОценок пока нет
- Olson, Dennis - Dennis Olson For Representative - 1920 - D - DebtsДокумент1 страницаOlson, Dennis - Dennis Olson For Representative - 1920 - D - DebtsZach EdwardsОценок пока нет
- Olson, Dennis - Dennis Olson For Representative - 1920 - E - in - KindДокумент1 страницаOlson, Dennis - Dennis Olson For Representative - 1920 - E - in - KindZach EdwardsОценок пока нет
- Olson, Dennis - Dennis Olson For Representative - 1920 - DR1 - 04-26-2010Документ2 страницыOlson, Dennis - Dennis Olson For Representative - 1920 - DR1 - 04-26-2010Zach EdwardsОценок пока нет
- Ravi Panwar FIIB CIP-2019-Report PDFДокумент53 страницыRavi Panwar FIIB CIP-2019-Report PDFRavi SinghОценок пока нет
- Banking-Theory-Law and PracticeДокумент258 страницBanking-Theory-Law and PracticeRahul Sharma100% (1)
- Pak Enings HTДокумент15 страницPak Enings HTVincent SampianoОценок пока нет
- CFAS Notes (1st Year)Документ66 страницCFAS Notes (1st Year)kookie bunnyОценок пока нет
- Nego Foreign JurisДокумент21 страницаNego Foreign JurisKristine ComaОценок пока нет
- Unclaimed Property LawsДокумент48 страницUnclaimed Property LawsMichelle Morgan LongstrethОценок пока нет
- FDFGДокумент3 страницыFDFGHemanth DevaiahОценок пока нет
- Functions of Commercial BanksДокумент23 страницыFunctions of Commercial BanksAaradhya MestryОценок пока нет
- CBSE Class 10 Social Science Chapter-3 Money and Credit NotesДокумент4 страницыCBSE Class 10 Social Science Chapter-3 Money and Credit NotesVishrut Shahi100% (1)
- Fundamental of Banking MarathiДокумент256 страницFundamental of Banking MarathiAtulОценок пока нет
- Samsung CaseДокумент3 страницыSamsung CaseBlessОценок пока нет
- Report On Dutch Bangla Bank Ratio AnalysisДокумент32 страницыReport On Dutch Bangla Bank Ratio AnalysisMishuОценок пока нет
- Rastriye Banijye BankДокумент7 страницRastriye Banijye BankAadarsh UpretiОценок пока нет
- Commercial Banking: Chapter ThreeДокумент39 страницCommercial Banking: Chapter ThreeYoseph KassaОценок пока нет
- Data Analysis On Financial InclusionДокумент21 страницаData Analysis On Financial InclusionHeidi Bell50% (2)
- Cash and Cash EquivalentsДокумент20 страницCash and Cash EquivalentsPetrina100% (1)
- 4542 Finacle Custom Menu OptionДокумент21 страница4542 Finacle Custom Menu OptionTarundeep KaurОценок пока нет
- Class DiagramДокумент2 страницыClass DiagramJongОценок пока нет
- Industrial FinanceДокумент11 страницIndustrial Financedesaijpr90% (10)
- Professional Banker Certificate - The Business of Banking and The Economic Environment (Chapter 1)Документ38 страницProfessional Banker Certificate - The Business of Banking and The Economic Environment (Chapter 1)KALKIDAN KASSAHUNОценок пока нет
- CASA'S KEY ROLE IN BANK PROFITABILITYДокумент30 страницCASA'S KEY ROLE IN BANK PROFITABILITYKshitij SharmaОценок пока нет
- Money, Banking and The Macro-Economy - Answers: 5.1 Checklist QuestionsДокумент8 страницMoney, Banking and The Macro-Economy - Answers: 5.1 Checklist QuestionscesarsaraujoОценок пока нет
- 10 Bank Reconciliation Statement-1Документ9 страниц10 Bank Reconciliation Statement-1Abdul SamadОценок пока нет
- Money As Debt - TranscriptДокумент7 страницMoney As Debt - TranscriptWherethestreets HavenonameОценок пока нет
- Solidbank Corp. vs. ArrietaДокумент6 страницSolidbank Corp. vs. Arrietacogito110Оценок пока нет
- The Federal Reserve ActДокумент121 страницаThe Federal Reserve Actjram64100% (2)
- Report On AIBL (GB & FE)Документ78 страницReport On AIBL (GB & FE)Rayhan Zahid HasanОценок пока нет
- Banking Law Reviewer Hot JuristДокумент27 страницBanking Law Reviewer Hot Juristgrego centillas100% (1)