Вам также может понравиться
- Weeks 1-2 Carb Cycling Blueprint FINAL r1Документ24 страницыWeeks 1-2 Carb Cycling Blueprint FINAL r1Umashanker VishwakarmaОценок пока нет
- Who Rec For AncДокумент181 страницаWho Rec For AncDana Indania SariОценок пока нет
- Diabetes Mellitus Type 2Документ16 страницDiabetes Mellitus Type 2MTs MIFDAОценок пока нет
- Diabetes Mellitus and Oral Health: An Interprofessional ApproachОт EverandDiabetes Mellitus and Oral Health: An Interprofessional ApproachОценок пока нет
- Diabete Mellitus HandoutsДокумент7 страницDiabete Mellitus HandoutsSittie Nashieva A. UsmanОценок пока нет
- Type 2 Diabetes MellitusДокумент19 страницType 2 Diabetes MellitusFelipe Senn Guerrero100% (2)
- NCP: Diabetes Mellitus Prepregnancy/GestationalДокумент11 страницNCP: Diabetes Mellitus Prepregnancy/GestationalJavie85% (13)
- Discover Natural -Alternative Therapies for Managing Type 2 DiabetesОт EverandDiscover Natural -Alternative Therapies for Managing Type 2 DiabetesОценок пока нет
- Diabetic Ketoacidosis Written ReportДокумент19 страницDiabetic Ketoacidosis Written ReportEros Victorino100% (2)
- (MT6317) Unit 6.1 Introduction To Carbohydrates and Glucose DeterminationДокумент12 страниц(MT6317) Unit 6.1 Introduction To Carbohydrates and Glucose DeterminationJC DomingoОценок пока нет
- Oajbs Id 000530Документ8 страницOajbs Id 000530Aldy RanggaОценок пока нет
- Medical Clinics of North America Volume 101 Issue 3 2017 (Doi 10.1016 - J.mcna.2016.12.011) Fayfman, Maya Pasquel, Francisco J. Umpierrez, Guillermo E. - Management of Hyperglycemic CrisesДокумент20 страницMedical Clinics of North America Volume 101 Issue 3 2017 (Doi 10.1016 - J.mcna.2016.12.011) Fayfman, Maya Pasquel, Francisco J. Umpierrez, Guillermo E. - Management of Hyperglycemic CrisesBlanca Herrera MoralesОценок пока нет
- Hyperglycemic Crises in Adult Patients With DiabetesДокумент49 страницHyperglycemic Crises in Adult Patients With DiabetesrambuОценок пока нет
- Hyperglycaemic EmergenciesДокумент11 страницHyperglycaemic EmergenciesdramaysinghОценок пока нет
- Diabetes Emergencia Umpierrez 2016Документ11 страницDiabetes Emergencia Umpierrez 2016Nathalie GandoОценок пока нет
- Hyperglycemic CrisisДокумент9 страницHyperglycemic CrisisRoberto López MataОценок пока нет
- Diabetes: Introduction and History of The Diabetes MellitusДокумент6 страницDiabetes: Introduction and History of The Diabetes Mellitusثہيہودور'ۦ شہوأنہﮩٰۧٛۗ ﮩٰۧٛОценок пока нет
- Review: Orit Pinhas-Hamiel, Philip ZeitlerДокумент9 страницReview: Orit Pinhas-Hamiel, Philip ZeitlerNadhifaОценок пока нет
- Heart Failure in Type 2 Diabetes Mellitus.2019Документ21 страницаHeart Failure in Type 2 Diabetes Mellitus.2019Anonymous RJntvnОценок пока нет
- Management of Diabetic Ketoacidosis in Adults - A Narrative ReviewДокумент12 страницManagement of Diabetic Ketoacidosis in Adults - A Narrative Reviewghr9cjy5npОценок пока нет
- Diabetes 5Документ16 страницDiabetes 5patricia osei-owusuОценок пока нет
- Diabetes MellitusДокумент43 страницыDiabetes MellitusRobi HSОценок пока нет
- Dia Care 2009 Kitabchi 1335 43crisis HiperglicemicasДокумент9 страницDia Care 2009 Kitabchi 1335 43crisis HiperglicemicassstdocОценок пока нет
- Manejo de Crises HiperglicémicasДокумент1 страницаManejo de Crises HiperglicémicasWilson Lukeny G. JoséОценок пока нет
- Iabetes Ellitus: Section 7. Endocrinologic DisordersДокумент24 страницыIabetes Ellitus: Section 7. Endocrinologic DisordersAyoe SemangatzОценок пока нет
- AJGP 05 2019 Focus Willix Hyperglycaemic Presentations WEBДокумент5 страницAJGP 05 2019 Focus Willix Hyperglycaemic Presentations WEBmystatОценок пока нет
- Kidney ObeseДокумент18 страницKidney ObeseIrene KristiantiОценок пока нет
- Guideline ADA 2010 in Hyperglicemia CrisisДокумент9 страницGuideline ADA 2010 in Hyperglicemia CrisisAissyiyah Nur An NisaОценок пока нет
- PTJ 1254Документ11 страницPTJ 1254angsokasatuОценок пока нет
- DM Final PDFДокумент15 страницDM Final PDFgiftyОценок пока нет
- R VI W Li9'Ery1LqeДокумент28 страницR VI W Li9'Ery1LqeV.Bastin JeromeОценок пока нет
- Overview of The StudyДокумент11 страницOverview of The StudyNaveen rajОценок пока нет
- 2022 JAMA - Analysis of Severe Hypoglycemia Among Adults W - Type 2 Diabetes and Nonalcoholic Fatty Liver Disease (Lee) (R)Документ13 страниц2022 JAMA - Analysis of Severe Hypoglycemia Among Adults W - Type 2 Diabetes and Nonalcoholic Fatty Liver Disease (Lee) (R)Xavier Alexandro Ríos SalinasОценок пока нет
- Jurnal Kad Dan HonkДокумент9 страницJurnal Kad Dan Honksimpati91Оценок пока нет
- Diabetes y Patologias OralesДокумент11 страницDiabetes y Patologias OralesMedusa GorgonОценок пока нет
- Classification, Pathophysiology, Diagnosis and Management of DiabetesДокумент19 страницClassification, Pathophysiology, Diagnosis and Management of DiabeteswakhidrizkaОценок пока нет
- Pelumi 2Документ11 страницPelumi 2oluwasegunnathaniel0Оценок пока нет
- Diagnosis and Management of Hyperglycemic Emergencies: Hormones (Athens, Greece) October 2011Документ12 страницDiagnosis and Management of Hyperglycemic Emergencies: Hormones (Athens, Greece) October 2011nia rahayu wОценок пока нет
- A18 - KAD HHS - FullДокумент9 страницA18 - KAD HHS - FullMuhammad BilalОценок пока нет
- Hypoglycemia in Diabetes: P E. C, S N. D, H SДокумент11 страницHypoglycemia in Diabetes: P E. C, S N. D, H SFabio FabbriОценок пока нет
- Contents Treatment of Type 2 Diabetes MДокумент17 страницContents Treatment of Type 2 Diabetes MaveekumbharОценок пока нет
- jdn18 7 292 5Документ4 страницыjdn18 7 292 5Miladya RahmiОценок пока нет
- Diabetes MellitusДокумент58 страницDiabetes Mellitusanilkrganesh11Оценок пока нет
- Emerging Role of Dipeptidyl Peptidase-IV (DPP-4) Inhibitor Vildagliptin in The Management of Type 2 DiabetesДокумент9 страницEmerging Role of Dipeptidyl Peptidase-IV (DPP-4) Inhibitor Vildagliptin in The Management of Type 2 DiabetesIndrasuari Anak Agung AyuОценок пока нет
- Ehrmann 2020Документ11 страницEhrmann 2020miguelfilipegralhaalmeidaОценок пока нет
- ADA Type 2 Diabetes in ChildrensДокумент10 страницADA Type 2 Diabetes in ChildrensCho Maharani Rijhigo BaeОценок пока нет
- CHF Secondary To COPD and DM Type 2Документ3 страницыCHF Secondary To COPD and DM Type 2Ma Regina Ocio PatanaОценок пока нет
- Diabetes Mellitus Type 2Документ16 страницDiabetes Mellitus Type 2Roland Jireh MarananОценок пока нет
- HHS Public Access: Diabetes and Stroke: Epidemiology, Pathophysiology, Pharmaceuticals and OutcomesДокумент13 страницHHS Public Access: Diabetes and Stroke: Epidemiology, Pathophysiology, Pharmaceuticals and OutcomesayuОценок пока нет
- Hypoglycemia - 2014 Morales N DoronДокумент8 страницHypoglycemia - 2014 Morales N DoronDian Eka RamadhaniОценок пока нет
- Imune DeseaseДокумент6 страницImune DeseaseGeorge NicoloiuОценок пока нет
- Hypoglycemia, Diabetes, and Cardiovascular Events: C V. D, G B. B, V FДокумент6 страницHypoglycemia, Diabetes, and Cardiovascular Events: C V. D, G B. B, V FHervi LaksariОценок пока нет
- Low Hba1C and Increased Mortality Risk-Is Frailty A Confounding Factor?Документ9 страницLow Hba1C and Increased Mortality Risk-Is Frailty A Confounding Factor?Dayse OliveiraОценок пока нет
- Diabetic Research 22Документ33 страницыDiabetic Research 22Hakim KhanОценок пока нет
- The Two-Way Relationship Between Diabetes and Periodontal DiseaseДокумент12 страницThe Two-Way Relationship Between Diabetes and Periodontal DiseaseDevi AlfianiОценок пока нет
- Diabetes Mellitus: Insights From Epidemiology, Biochemistry, Risk Factors, Diagnosis, Complications and Comprehensive ManagementДокумент15 страницDiabetes Mellitus: Insights From Epidemiology, Biochemistry, Risk Factors, Diagnosis, Complications and Comprehensive Managementabdulqudus abdulsalamОценок пока нет
- Update On Diabetes Mellitus: Prevention, Treatment, and Association With Oral DiseasesДокумент10 страницUpdate On Diabetes Mellitus: Prevention, Treatment, and Association With Oral DiseasesAlexandra NinaОценок пока нет
- Assessment & Treatment of Diabetic Emergencies: Paramedic LevelДокумент12 страницAssessment & Treatment of Diabetic Emergencies: Paramedic LevelSarah-kate PatersonОценок пока нет
- Introduction To Diabetes Mellitus Epidemiology of Diabetes MellitusДокумент4 страницыIntroduction To Diabetes Mellitus Epidemiology of Diabetes MellitusMARK 365Оценок пока нет
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in AdultsДокумент17 страницDiabetic Ketoacidosis and Hyperosmolar Hyperglycemic State in Adultsjoseaugustorojas9414Оценок пока нет
- Emergency Medicine EducationHyperglycemic Hyperosmolar State: ED PRДокумент19 страницEmergency Medicine EducationHyperglycemic Hyperosmolar State: ED PRSyed Shahrul Naz SyedОценок пока нет
- Polypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 DiabetesДокумент12 страницPolypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 Diabetesapi-311409998Оценок пока нет
- ADA Consenssus DM Eldery 2012Документ15 страницADA Consenssus DM Eldery 2012Jason CarterОценок пока нет
- Compliance and Retention in CareДокумент45 страницCompliance and Retention in Carewangdavou08Оценок пока нет
- Discover The Best Exercises For Overall Health & Longevity - Based On The Teachings Of Dr. Andrew Huberman: The Ultimate Workout Guide For Lifelong Well-BeingОт EverandDiscover The Best Exercises For Overall Health & Longevity - Based On The Teachings Of Dr. Andrew Huberman: The Ultimate Workout Guide For Lifelong Well-BeingОценок пока нет
- Prediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalОт EverandPrediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalОценок пока нет
- Case 3 Care of Client With GI, PUD, Cancer, Liver FailureДокумент33 страницыCase 3 Care of Client With GI, PUD, Cancer, Liver FailureNyeam NyeamОценок пока нет
- Interactive Patient Case Management #1Документ33 страницыInteractive Patient Case Management #1Luzman HizrianОценок пока нет
- Early - Detection - and - Management DMT2Документ35 страницEarly - Detection - and - Management DMT2AlfajridrgОценок пока нет
- Kel 4 2020 Efficacy and Safety of Use of The Fasting AlgorithmДокумент9 страницKel 4 2020 Efficacy and Safety of Use of The Fasting AlgorithmBima Gewab Tjah RastafaraОценок пока нет
- Carb Counting Type1Документ22 страницыCarb Counting Type1Dhanalakshmi ThiyagarajanОценок пока нет
- The Diabetes MiracleДокумент8 страницThe Diabetes MiracleOWOLABIОценок пока нет
- PedomanДокумент2 страницыPedomanandi namirahОценок пока нет
- A Plant Review Butea Monosperma (Lam.) KuntzeДокумент15 страницA Plant Review Butea Monosperma (Lam.) KuntzeNadeemОценок пока нет
- 1 399A Prime ElectrolyteДокумент2 страницы1 399A Prime ElectrolyteNessma EmadОценок пока нет
- Diet, Insulin and Blood Glucose: © Food - A Fact of Life 2009Документ22 страницыDiet, Insulin and Blood Glucose: © Food - A Fact of Life 2009Eliana MuisОценок пока нет
- Hypoglycemic Property of Insulin PlantДокумент50 страницHypoglycemic Property of Insulin Plantanaceto dialino0% (2)
- Hubungan Tingkat StresДокумент8 страницHubungan Tingkat StresAri SuhartantoОценок пока нет
- NCM 116 Skills - Midterm NotesДокумент20 страницNCM 116 Skills - Midterm NotesmareginaОценок пока нет
- The Journal For Nurse Practitioners: Jacqueline O'Toole, MSC, NP, Irene Gibson, Ma, RGN, Gerard T. Flaherty, MDДокумент4 страницыThe Journal For Nurse Practitioners: Jacqueline O'Toole, MSC, NP, Irene Gibson, Ma, RGN, Gerard T. Flaherty, MDGina GuisamanoОценок пока нет
- BSN 2B 2d CASE STUDY FinalДокумент35 страницBSN 2B 2d CASE STUDY Finalann camposОценок пока нет
- Expanded National Nutrition Survey: 2019 Results: Health and Nutritional Status of Filipino Adults, 20-59 Years OldДокумент61 страницаExpanded National Nutrition Survey: 2019 Results: Health and Nutritional Status of Filipino Adults, 20-59 Years Oldzvfvr95hrkОценок пока нет
- Hyperglycemia Algorithm 2Документ1 страницаHyperglycemia Algorithm 2damondouglasОценок пока нет
- Cactus (Opuntia Ficus-Indica) : A Review On Its Antioxidants Properties and Potential Pharmacological Use in Chronic DiseasesДокумент9 страницCactus (Opuntia Ficus-Indica) : A Review On Its Antioxidants Properties and Potential Pharmacological Use in Chronic DiseasesAidОценок пока нет
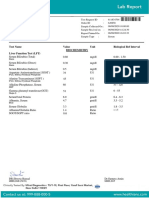
- Test Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Документ7 страницTest Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Himanshu GarkhelОценок пока нет
- File - 20220320 - 212040 - QC1 1134uc 2022-11Документ5 страницFile - 20220320 - 212040 - QC1 1134uc 2022-11Đạt Trần TiếnОценок пока нет
- HgbA1c 11 24 09 - 0 PDFДокумент2 страницыHgbA1c 11 24 09 - 0 PDFekorahmanadiОценок пока нет
- Week 2 - Drugs and The BodyДокумент18 страницWeek 2 - Drugs and The BodyDino MicaОценок пока нет
- Ap BioДокумент34 страницыAp BiotehilashiftehОценок пока нет
- Traditional Medicinal Uses and Therapeutic Benefits of Momordica Charantia LinnДокумент6 страницTraditional Medicinal Uses and Therapeutic Benefits of Momordica Charantia Linnjuan mezaОценок пока нет