Вам также может понравиться
- Procedure Checklist Chapter 19: Assessing The Chest and LungsДокумент2 страницыProcedure Checklist Chapter 19: Assessing The Chest and LungsjthsОценок пока нет
- Medical Surgical Nursing PinoyДокумент85 страницMedical Surgical Nursing PinoyrosebaseОценок пока нет
- Evaluation Checklist Case 7 Bronchial AsthmaДокумент7 страницEvaluation Checklist Case 7 Bronchial AsthmaChristian MendiolaОценок пока нет
- Patients With Hearing and Balance DisordersДокумент33 страницыPatients With Hearing and Balance Disordershalloween candyОценок пока нет
- Past MCQs On Ocular AnatomyДокумент7 страницPast MCQs On Ocular AnatomyEliza Spark33% (6)
- Cranial Nerve AssessmentДокумент5 страницCranial Nerve AssessmentBAdz TanОценок пока нет
- Splinting InstructionsДокумент19 страницSplinting Instructionsiris_madrigal100% (1)
- Human Nervous-SystemДокумент32 страницыHuman Nervous-SystemhwzeeeОценок пока нет
- OB Care Map L&DДокумент3 страницыOB Care Map L&DYasmin Santibañez100% (1)
- Care of Pediatric Client With Dermatologic DisorderДокумент3 страницыCare of Pediatric Client With Dermatologic DisorderAraw GabiОценок пока нет
- Spina BifidaДокумент2 страницыSpina BifidaTracy100% (2)
- Cranial Nerve AssessmentДокумент4 страницыCranial Nerve AssessmentAnonymous h2EnKyDbОценок пока нет
- Cranial Nerve ExaminationДокумент3 страницыCranial Nerve ExaminationtomodachiОценок пока нет
- PRESBYCUSISДокумент43 страницыPRESBYCUSISDesiana AyuОценок пока нет
- Cranial Nerves SummaryДокумент3 страницыCranial Nerves SummaryJoash F. Pacquing75% (4)
- Complications of FracturesДокумент13 страницComplications of FracturesmilananandОценок пока нет
- Head To Toe Assessment Guide ToolДокумент3 страницыHead To Toe Assessment Guide Toolkezia_lillyОценок пока нет
- Introduction To General AnatomyДокумент7 страницIntroduction To General AnatomyPia Abila100% (1)
- Cranial NervesДокумент14 страницCranial NervesIrina Garlea-Robu100% (1)
- Medical Cartoon and The AwesomeДокумент2 страницыMedical Cartoon and The Awesomekrrishshrish140% (1)
- 12 Cranial Nerves: By: Dr. Pamela Josefina T. FabieДокумент48 страниц12 Cranial Nerves: By: Dr. Pamela Josefina T. FabieAbdullah Saleem100% (3)
- Head To Toe Physical Assessment: College of NursingДокумент4 страницыHead To Toe Physical Assessment: College of NursingMaicah ShaneОценок пока нет
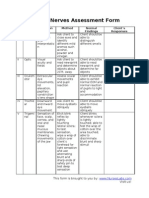
- Cranial Nerves Assessment FormДокумент3 страницыCranial Nerves Assessment Formmhel03_chickmagnetОценок пока нет
- 12 Cranial NervesДокумент2 страницы12 Cranial NervesJessica KruppОценок пока нет
- Pupil Respose AssessmentДокумент4 страницыPupil Respose AssessmentRrichard Prieto MmallariОценок пока нет
- Abdominal Assessment VideoДокумент4 страницыAbdominal Assessment VideoAmber Nicole HubbardОценок пока нет
- Developmental Stages - Infant To AdolescentДокумент6 страницDevelopmental Stages - Infant To AdolescentGeguirra, Michiko SarahОценок пока нет
- Summary of Cranial NervesДокумент1 страницаSummary of Cranial NervesjackieОценок пока нет
- Session 2 Memorization Hacks in Nursing & Learning About Meal PlanДокумент69 страницSession 2 Memorization Hacks in Nursing & Learning About Meal Planataraxialli100% (1)
- Anatomy and Physiology of The BRAINДокумент5 страницAnatomy and Physiology of The BRAING FernandezОценок пока нет
- Concept Map FinalДокумент1 страницаConcept Map Finalapi-383763177Оценок пока нет
- NANDA DX NI, NOДокумент165 страницNANDA DX NI, NOKerry Brown100% (1)
- Head Injury Management of PediatricДокумент22 страницыHead Injury Management of PediatricIrma KusumaОценок пока нет
- Head To Toe AssessmentДокумент22 страницыHead To Toe AssessmentNessa Layos MorilloОценок пока нет
- Screening Head To Toe Physical ExaminationДокумент16 страницScreening Head To Toe Physical ExaminationJay Mar Mendoza BabateОценок пока нет
- Thoracentesis Is Also Known As Pleural Fluid AnalysisДокумент3 страницыThoracentesis Is Also Known As Pleural Fluid AnalysisJ.r. MercadoОценок пока нет
- Cranial NervesДокумент67 страницCranial NervesBahaa ShaabanОценок пока нет
- Nursing Assessment in Tabular Form (Repaired) To Be Placed!@#%$!@# #@ @Документ5 страницNursing Assessment in Tabular Form (Repaired) To Be Placed!@#%$!@# #@ @Leo Buquiran AcabalОценок пока нет
- LaminectomyДокумент5 страницLaminectomyanon_931797817Оценок пока нет
- Compartment Syndrome: Return To TopДокумент3 страницыCompartment Syndrome: Return To TopSania Kamal BalweelОценок пока нет
- Caring For A CastДокумент39 страницCaring For A CastGrape JuiceОценок пока нет
- Intramuscular Injection GuidelinesДокумент2 страницыIntramuscular Injection Guidelinesangie10231Оценок пока нет
- MASTOIDECTOMY Written OutputДокумент3 страницыMASTOIDECTOMY Written OutputJoe RealОценок пока нет
- Health HistoryДокумент7 страницHealth HistoryAnnapurna DangetiОценок пока нет
- Med Surg Chapter 1Документ2 страницыMed Surg Chapter 1Judy072100% (1)
- Table of Cranial NervesДокумент7 страницTable of Cranial NervesCoy EnОценок пока нет
- Growth and Development Growing Complex Phenomenon of A Structure or Whole GrowthДокумент69 страницGrowth and Development Growing Complex Phenomenon of A Structure or Whole GrowthYna RamiroОценок пока нет
- Swallowing MechanismДокумент6 страницSwallowing MechanismLittle MummutОценок пока нет
- Spinal Cord Injury: Mrs. Zaida ZaracenaДокумент36 страницSpinal Cord Injury: Mrs. Zaida ZaracenaArdhel LoslosoОценок пока нет
- Thoracic and Lung Assessment: Physical Examination of The Thorax and The LungsДокумент16 страницThoracic and Lung Assessment: Physical Examination of The Thorax and The Lungsshannon c. lewis100% (1)
- Pulmonary Edema: Topic OutlineДокумент2 страницыPulmonary Edema: Topic OutlineKdamnz100% (1)
- Pain OldДокумент16 страницPain OldgireeshsachinОценок пока нет
- Use The Following Criteria in Evaluating The Skill PerformanceДокумент4 страницыUse The Following Criteria in Evaluating The Skill Performancekookie100% (1)
- During The CCA Exam. Please Note You Are Responsible For The Content Knowledge of Items Without An Asterisk That May Be Present On The Written Exam.Документ2 страницыDuring The CCA Exam. Please Note You Are Responsible For The Content Knowledge of Items Without An Asterisk That May Be Present On The Written Exam.helamahjoubmounirdmoОценок пока нет
- Anatomy & Physiology 1 Chapter 9 The Nervous System Flashcards - QuizletДокумент7 страницAnatomy & Physiology 1 Chapter 9 The Nervous System Flashcards - Quizletmalenya1100% (1)
- Chapter 30: Health Assessment and Physical Examination: Test BankДокумент23 страницыChapter 30: Health Assessment and Physical Examination: Test BankNurse UtopiaОценок пока нет
- Health Assessment Complete 2Документ14 страницHealth Assessment Complete 2kimberly100% (1)
- Inflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandInflamed Trachea, (Tracheitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Epistaxis (Nose Bleed), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandEpistaxis (Nose Bleed), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Nasal and Paranasal Sinus PathologiesДокумент7 страницNasal and Paranasal Sinus Pathologiespunct_org3256Оценок пока нет
- Health Assessment Checklist Week1 and 2Документ7 страницHealth Assessment Checklist Week1 and 2Wylyn Mae VisqueraОценок пока нет
- What Does Your "Homunculus" Look Like?: Mapping Your Brain PurposeДокумент3 страницыWhat Does Your "Homunculus" Look Like?: Mapping Your Brain PurposeClarissa PottsОценок пока нет
- Checklist Nematoda Zootaxa 2011Документ88 страницChecklist Nematoda Zootaxa 2011Ana CarolinaОценок пока нет
- The Neck / Firas Al-Hameed by Rusul AnwarДокумент7 страницThe Neck / Firas Al-Hameed by Rusul Anwarزين العابدين محمد عويشОценок пока нет
- Combining Millard's and Cronin's Methods of Unilateral Cleft Lip Repair - A Comparative StudyДокумент5 страницCombining Millard's and Cronin's Methods of Unilateral Cleft Lip Repair - A Comparative StudyDrDejanDrakulОценок пока нет
- Verpaele 2015Документ9 страницVerpaele 2015Rafał PokrowieckiОценок пока нет
- Text Za Stranu 1Документ2 страницыText Za Stranu 1Zagor Te NejОценок пока нет
- Biological Psychology Lesson 5 NotesДокумент24 страницыBiological Psychology Lesson 5 Notesjeyn100% (1)
- Pictorial Essay: Anatomical Variations of Paranasal Sinuses On Multidetector Computed Tomography-How Does It Help FESS Surgeons?Документ8 страницPictorial Essay: Anatomical Variations of Paranasal Sinuses On Multidetector Computed Tomography-How Does It Help FESS Surgeons?claragustin_53768590Оценок пока нет
- Shunt Exposure As A Ventriculoperitoneal Shunt Complication A CaseДокумент8 страницShunt Exposure As A Ventriculoperitoneal Shunt Complication A CasePutri Tamara DasantosОценок пока нет
- Anatomy of The Left EyeДокумент3 страницыAnatomy of The Left EyeJaessa FelicianoОценок пока нет
- Topic 2 - Part 2 - Work Environment Design - Auditory SenseДокумент57 страницTopic 2 - Part 2 - Work Environment Design - Auditory SenseCamille AmparoОценок пока нет
- The Nasolabial Fla - 2003 - Oral and Maxillofacial Surgery Clinics of North AmerДокумент9 страницThe Nasolabial Fla - 2003 - Oral and Maxillofacial Surgery Clinics of North Amerlaljadeff12Оценок пока нет
- Bio 109 Module 4Документ18 страницBio 109 Module 4Marites Maylanon0% (1)
- Lesson 1 CT Scan BasicДокумент5 страницLesson 1 CT Scan BasicPauline BurgosОценок пока нет
- Arterial Supply of Head and NeckДокумент41 страницаArterial Supply of Head and NeckKhadija Vasi100% (1)
- Ebbesson, Sven O. E. (1980) - Comparative Neurology of The Telencephalon. The Telencephalon of SnakesДокумент39 страницEbbesson, Sven O. E. (1980) - Comparative Neurology of The Telencephalon. The Telencephalon of SnakesLivia PereiraОценок пока нет
- Surgical Ii Case StudyДокумент9 страницSurgical Ii Case StudyRomuel PaparonОценок пока нет
- Review of Cerebral Anatomy:: DiencephalonДокумент27 страницReview of Cerebral Anatomy:: DiencephalonEJ GejonОценок пока нет
- Cranial NervesДокумент118 страницCranial NervesGan'sОценок пока нет
- Assessing The Ears and Hearing Acuity: Return Demonstration Tool Evaluation ForДокумент3 страницыAssessing The Ears and Hearing Acuity: Return Demonstration Tool Evaluation Forclint xavier odangoОценок пока нет
- Head To Neck Health AssessmentДокумент6 страницHead To Neck Health AssessmentKathrina Doroneo (rina)Оценок пока нет
- Dr. Rahmi Ardhini, SPSДокумент60 страницDr. Rahmi Ardhini, SPSsatyagraha84Оценок пока нет
- Bilingual-Paper WДокумент4 страницыBilingual-Paper WzОценок пока нет
- Head and Neck Radiology: Skull X-RayДокумент20 страницHead and Neck Radiology: Skull X-RayadiningtitisОценок пока нет
- 3 - Head Injured PatientДокумент94 страницы3 - Head Injured PatientAmmarОценок пока нет
- Name: Pius Troy Macapaz Section: BSN-III N32: Neurologic Assessment QuizДокумент3 страницыName: Pius Troy Macapaz Section: BSN-III N32: Neurologic Assessment QuizYamete KudasaiОценок пока нет