Вам также может понравиться
- Endodontic RadiologyОт EverandEndodontic RadiologyBettina BasraniОценок пока нет
- Test Bank For Essentials of Pathophysiology 3rd Edition, PorthДокумент23 страницыTest Bank For Essentials of Pathophysiology 3rd Edition, PorthILL110100% (1)
- Joels Lecture Surgical EndodonticsДокумент105 страницJoels Lecture Surgical Endodonticsjoel devaraj100% (2)
- Diagnostic Aids in Endodontics AbhiДокумент32 страницыDiagnostic Aids in Endodontics AbhiJitender Reddy100% (1)
- Magnification in EndodonticsДокумент53 страницыMagnification in Endodonticsdurga7100% (1)
- A Review On Success and Failure in EndodonticДокумент25 страницA Review On Success and Failure in EndodonticjyotsnasistlaОценок пока нет
- PERFORATIONS & MANAGEMENT: A REVIEW OF DIAGNOSIS AND TREATMENTДокумент163 страницыPERFORATIONS & MANAGEMENT: A REVIEW OF DIAGNOSIS AND TREATMENTAPARNA AARATHI SREEKUMARОценок пока нет
- Non-Carious Tooth Surface Loss Causes and TreatmentsДокумент18 страницNon-Carious Tooth Surface Loss Causes and TreatmentsAjmal NajeebОценок пока нет
- Human Body Revision NotesДокумент83 страницыHuman Body Revision NotesdoaaОценок пока нет
- Endodontic SurgeryДокумент16 страницEndodontic SurgeryauntymayaОценок пока нет
- Avoiding and Treating Dental Complications: Best Practices in DentistryОт EverandAvoiding and Treating Dental Complications: Best Practices in DentistryDeborah A. TermeieОценок пока нет
- Treatment Planning Single Maxillary Anterior Implants for DentistsОт EverandTreatment Planning Single Maxillary Anterior Implants for DentistsОценок пока нет
- Cleaning and Shaping TechniquesДокумент26 страницCleaning and Shaping TechniquesRohan Bhagat100% (1)
- Slides 6 - ObturationДокумент22 страницыSlides 6 - Obturationبراءة أحمد السلاماتОценок пока нет
- Asepsis in EndodonticsДокумент55 страницAsepsis in EndodonticsVidya AnandОценок пока нет
- Recent Advances in CompositesДокумент6 страницRecent Advances in Compositesanshumankhaitan100% (1)
- Obturation MaterialsДокумент47 страницObturation MaterialsCraig Lee100% (2)
- Recent Advances in Endodontic Instruments / Orthodontic Courses by Indian Dental AcademyДокумент20 страницRecent Advances in Endodontic Instruments / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- New Advances in Caries RemovalДокумент45 страницNew Advances in Caries Removalyogi_2311Оценок пока нет
- C Shaped CanalsДокумент33 страницыC Shaped CanalsFahad QiamОценок пока нет
- Rotary EndodonticsДокумент61 страницаRotary EndodonticsVijayendra kamathОценок пока нет
- Flare Ups in EndodonticsДокумент12 страницFlare Ups in EndodonticsAnamika Thakur RanaОценок пока нет
- Rotary Instrumentation Using 1Документ41 страницаRotary Instrumentation Using 1sai GanapathyОценок пока нет
- Smear LayerДокумент36 страницSmear LayerNaomi SinghОценок пока нет
- Recent Advances in Composites PDFДокумент7 страницRecent Advances in Composites PDFShriya Shahu100% (1)
- 13 6 Endodontic Mishaps PDFДокумент20 страниц13 6 Endodontic Mishaps PDFzaheerbdsОценок пока нет
- Slide - 11 - Procedural AccidentsДокумент31 страницаSlide - 11 - Procedural AccidentsCWT2010100% (1)
- ACCESS CAVITY PREPARATION AnjaliДокумент69 страницACCESS CAVITY PREPARATION Anjalianjali sОценок пока нет
- Single Visit ClassДокумент42 страницыSingle Visit ClassNandita HegdeОценок пока нет
- Obturation of Root Canal LectureДокумент8 страницObturation of Root Canal LectureOsama AsadiОценок пока нет
- Rationale of Endodontic TreatmentДокумент45 страницRationale of Endodontic TreatmentAmy Rita0% (1)
- Cast RestorationsДокумент185 страницCast Restorationsrasagna reddyОценок пока нет
- Pulpoperiodontal Lesions..Документ39 страницPulpoperiodontal Lesions..SusanОценок пока нет
- Australian Dental Journal Research Supplement 2011Документ57 страницAustralian Dental Journal Research Supplement 2011Esha AroraОценок пока нет
- Objectives and techniques for determining working length in endodontic treatmentДокумент47 страницObjectives and techniques for determining working length in endodontic treatmentdrmahmoudbadrОценок пока нет
- 5.wonderful World of Endodontic Working Width The Forgotten Dimension - A ReviewДокумент7 страниц5.wonderful World of Endodontic Working Width The Forgotten Dimension - A ReviewSiva Kumar100% (1)
- Minimal Intervention DentistryДокумент76 страницMinimal Intervention DentistryRishab Sharma100% (1)
- Single Visit Endodontic TherapyДокумент95 страницSingle Visit Endodontic TherapyAshish Bhadane100% (2)
- Endodontic InsrumentДокумент52 страницыEndodontic InsrumentSawsan Z. JwaiedОценок пока нет
- Microbiology Aspect in EndodonticsДокумент80 страницMicrobiology Aspect in Endodonticswhussien7376100% (1)
- ACCESS CAVITY PREPARATION GUIDELINESДокумент35 страницACCESS CAVITY PREPARATION GUIDELINESShaheen Aboobacker Reniya ShaheenОценок пока нет
- Management of Badly Broken Down Teeth IIДокумент63 страницыManagement of Badly Broken Down Teeth IIAhmad Zuhdi Aljedi100% (7)
- Recent Advances in Caries Diagnosis Corrected TodayДокумент36 страницRecent Advances in Caries Diagnosis Corrected Todaydrprabhatsaxena91% (11)
- Microfilled Composite and Hybrid CompositeДокумент40 страницMicrofilled Composite and Hybrid CompositeMei XiaoОценок пока нет
- Aae Endodonticglossary2016Документ50 страницAae Endodonticglossary2016h20pologtОценок пока нет
- Preliminary ConsiderationsДокумент22 страницыPreliminary ConsiderationsDayen LimОценок пока нет
- Endo ObturationДокумент83 страницыEndo ObturationBețiu CornelОценок пока нет
- Failures of Root Canal TreatmentДокумент77 страницFailures of Root Canal Treatmenthardeep kaurОценок пока нет
- Obturation Techniques and DevicesДокумент29 страницObturation Techniques and DevicesArivinthaan Tanigajalam100% (1)
- Endodontic MishapsДокумент41 страницаEndodontic MishapsDrKaran Khaneja100% (4)
- Irrigant Delivery SystemsДокумент54 страницыIrrigant Delivery SystemsVimalKumarОценок пока нет
- DR Deepti Saini School of Dental Sciences USMДокумент36 страницDR Deepti Saini School of Dental Sciences USMLow Junfay Mark50% (2)
- Clinical Techniques of Direct Composite Resin and Glass Ionomer RestorationsДокумент79 страницClinical Techniques of Direct Composite Resin and Glass Ionomer RestorationsVidhi Thakur100% (1)
- Lecture 4 Diagnosis of Dental CariesДокумент12 страницLecture 4 Diagnosis of Dental CariesDt omarОценок пока нет
- Failures of Restorations / Orthodontic Courses by Indian Dental AcademyДокумент44 страницыFailures of Restorations / Orthodontic Courses by Indian Dental Academyindian dental academyОценок пока нет
- Management of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearДокумент44 страницыManagement of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearANUBHAОценок пока нет
- Cleaning and Shaping of The Root CanalДокумент96 страницCleaning and Shaping of The Root CanalSAICHARAN GОценок пока нет
- Cavosurface Treatment of Various RestorationДокумент29 страницCavosurface Treatment of Various RestorationRimjhim JainОценок пока нет
- Tooth Morphology and Access Cavity PreparationДокумент232 страницыTooth Morphology and Access Cavity Preparationusmanhameed8467% (3)
- Platelet CasesДокумент13 страницPlatelet CasesRaheel IftikharОценок пока нет
- Lesson 24Документ16 страницLesson 24Anshika BhargavaОценок пока нет
- Index in Platelet Aggregation Analysis Fea and Effect Antiplatelet TherapiesДокумент9 страницIndex in Platelet Aggregation Analysis Fea and Effect Antiplatelet Therapiesiq_dianaОценок пока нет
- Peptalk Proto Donation ProcДокумент61 страницаPeptalk Proto Donation ProcsunshineОценок пока нет
- HashbrownДокумент22 страницыHashbrownLeomill MendiolaОценок пока нет
- Clinical Protocol in Pediatrics, 2012Документ96 страницClinical Protocol in Pediatrics, 2012floare de colt100% (1)
- Approach To Coagulation DisordersДокумент20 страницApproach To Coagulation DisordersTri P BukerОценок пока нет
- SDCEP Anticoagulants GuidanceДокумент52 страницыSDCEP Anticoagulants GuidanceShlomit Zuñiga100% (1)
- CVD BleedДокумент25 страницCVD BleedArla Donissa-Donique Castillon Alvior100% (1)
- Xi. Clotting Time Bleeding TimeДокумент16 страницXi. Clotting Time Bleeding TimeCookie MonsterОценок пока нет
- DR Katek BalapalaДокумент73 страницыDR Katek BalapalaNathan LupiyaОценок пока нет
- Acute Inflammation: Rino Pattiata Dept. Patologi Anatomik FKUI JakartaДокумент48 страницAcute Inflammation: Rino Pattiata Dept. Patologi Anatomik FKUI JakartaRaja DarmawanОценок пока нет
- Blood Smear Basics 2016Документ18 страницBlood Smear Basics 2016anggaririnОценок пока нет
- Examination of Bacterial Contamination in Blood ComponentsДокумент21 страницаExamination of Bacterial Contamination in Blood ComponentsCik KahadiОценок пока нет
- Pharmacology of AutacoidsДокумент13 страницPharmacology of AutacoidsInocenteОценок пока нет
- Compilation of Patho 1ST Ia QuesДокумент46 страницCompilation of Patho 1ST Ia QuesseadiabaОценок пока нет
- General Surgery MCQДокумент190 страницGeneral Surgery MCQلمسة مصمم100% (1)
- Blood DonationДокумент24 страницыBlood DonationVivek30121982100% (1)
- Alteration of blood coagulation in CKD patients on dialysisДокумент26 страницAlteration of blood coagulation in CKD patients on dialysissubankar NagОценок пока нет
- Pre Analytical Clot EdДокумент12 страницPre Analytical Clot EdAnonymous w4qodCJОценок пока нет
- Hematologic DisorderДокумент16 страницHematologic Disorderjulesubayubay5428Оценок пока нет
- Hemodynamic Disorders-RevisedДокумент118 страницHemodynamic Disorders-Revisedspringding0% (1)
- Nursing Clients With Hematologic DisordersДокумент4 страницыNursing Clients With Hematologic DisordersLuna MarieОценок пока нет
- RBC Disorders, Bleeding Disorders, and Pharmacology ReviewДокумент11 страницRBC Disorders, Bleeding Disorders, and Pharmacology ReviewSyed Muhammad HameemОценок пока нет
- HaematologyReport PDFДокумент78 страницHaematologyReport PDFhamody662002Оценок пока нет
- Hemapheresis: Sandhya R. Panch and Harvey G. KleinДокумент11 страницHemapheresis: Sandhya R. Panch and Harvey G. KleinNur Melani Sari WardaniОценок пока нет
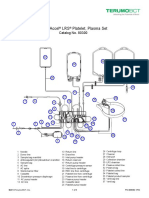
- Trima Accel LRS Platelet, Plasma Set: Catalog No. 80300Документ10 страницTrima Accel LRS Platelet, Plasma Set: Catalog No. 80300Suneo HonekawaОценок пока нет
- (Amaleaks - Blogspot.com) Eapp-111 Week 20 Second Quarter ExamДокумент35 страниц(Amaleaks - Blogspot.com) Eapp-111 Week 20 Second Quarter ExamGiovanni Hanz Rosales0% (1)