Вам также может понравиться
- Nursing Care Plan For Ineffective Tissue PerfusionДокумент19 страницNursing Care Plan For Ineffective Tissue Perfusionbrenhood78% (9)
- Nursing Note Sample 02Документ3 страницыNursing Note Sample 02okokokkkОценок пока нет
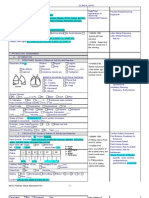
- Head To Toe Patient Assessment PDFДокумент2 страницыHead To Toe Patient Assessment PDFJesha PlatigueОценок пока нет
- Name of Patient:: DX: Ductal Carcino MA Right Side CC: Brest Mass DATДокумент2 страницыName of Patient:: DX: Ductal Carcino MA Right Side CC: Brest Mass DATdaliaОценок пока нет
- Delacruz 0Документ58 страницDelacruz 0Katrina CaveОценок пока нет
- Post Anesthesia Care Unit RecordДокумент1 страницаPost Anesthesia Care Unit RecordDamien Marwein100% (1)
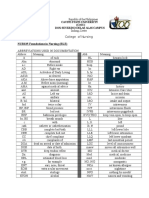
- Angeles University Foundation: A. Commonly Used Abbreviations Abbreviation English MeaningДокумент4 страницыAngeles University Foundation: A. Commonly Used Abbreviations Abbreviation English MeaningJaillah Reigne CuraОценок пока нет
- Abbreviations Used in DocumentationДокумент6 страницAbbreviations Used in DocumentationHydra Olivar - PantilganОценок пока нет
- Post-Anesthesia Record: Patient'S Name: Age: Sex: Attending PhysicianДокумент1 страницаPost-Anesthesia Record: Patient'S Name: Age: Sex: Attending PhysicianAina HaravataОценок пока нет
- Form1583A NewbornRecord1and2Документ4 страницыForm1583A NewbornRecord1and2miguealliОценок пока нет
- Common Abbreviations For The Patient Note USMLE Step 2CSДокумент1 страницаCommon Abbreviations For The Patient Note USMLE Step 2CSTiondi francisОценок пока нет
- Effective Airway ClearanceДокумент2 страницыEffective Airway ClearanceJoanna Mae CarolinoОценок пока нет
- Burn Patient Assessment and Management PlanДокумент5 страницBurn Patient Assessment and Management PlanChloe GoteraОценок пока нет
- Anesthesia Record 5-2Документ1 страницаAnesthesia Record 5-2Syed Raza Ali AbidiОценок пока нет
- Allll Exams Combinedd FinalДокумент14 страницAllll Exams Combinedd FinalAnshuОценок пока нет
- Head To Toe Patient AssessmentДокумент2 страницыHead To Toe Patient AssessmentJaypee Nuñez100% (2)
- Observational Patient Report Form PDFДокумент1 страницаObservational Patient Report Form PDFVictor PerdomoОценок пока нет
- Borja, Monica - EmrДокумент45 страницBorja, Monica - EmrMonica BorjaОценок пока нет
- Rlencm 107 Finals TransДокумент11 страницRlencm 107 Finals TransSachi Reuel BernateОценок пока нет
- Copy - of - AbbreviationsДокумент2 страницыCopy - of - Abbreviationsdhecht4000Оценок пока нет
- 3 MKD PEDIA QUICK NOTESДокумент37 страниц3 MKD PEDIA QUICK NOTESkaerickaericОценок пока нет
- Assessment Info NotesДокумент3 страницыAssessment Info NotesDiana DeckerОценок пока нет
- Code Blue Simulation TrainingДокумент26 страницCode Blue Simulation TrainingJenny CandraОценок пока нет
- Heada Lethar Irritab Crying Restles BulginДокумент2 страницыHeada Lethar Irritab Crying Restles BulginAdhaОценок пока нет
- Screenshot 2023-10-04 at 8.40.54 AmДокумент1 страницаScreenshot 2023-10-04 at 8.40.54 AmSage FlowerОценок пока нет
- Medical Form For NimДокумент1 страницаMedical Form For NimvishalОценок пока нет
- CC Concept MapДокумент5 страницCC Concept Mapapi-662323379Оценок пока нет
- SHOCK Slide WorkbookДокумент10 страницSHOCK Slide WorkbookPATHMAPRIYA GANESANОценок пока нет
- GI Skin GI Skin: Last BM Last BMДокумент2 страницыGI Skin GI Skin: Last BM Last BMlmaoheartsОценок пока нет
- Abbreviations TipДокумент3 страницыAbbreviations TipRegi Rusky Jasper100% (1)
- Pulmonary Edema: Mycobacterium Tuberculosis Patient BackgroundДокумент1 страницаPulmonary Edema: Mycobacterium Tuberculosis Patient BackgroundAubrey RecierdoОценок пока нет
- Warning: Learners, Please Complete The Learner Survey (Ucalgary - Ca/Codeblue/Surveys) Before Viewing This PowerpointДокумент27 страницWarning: Learners, Please Complete The Learner Survey (Ucalgary - Ca/Codeblue/Surveys) Before Viewing This PowerpointHandrian RahmanОценок пока нет
- IM - AcolДокумент4 страницыIM - AcolHomura Ch.Оценок пока нет
- NeralДокумент9 страницNeralmmОценок пока нет
- Annex (1) Health Check-Up Form: Detailed Candidate ReportДокумент6 страницAnnex (1) Health Check-Up Form: Detailed Candidate ReportMukesh MistriОценок пока нет
- Pharm Math and PharmacologyДокумент1 страницаPharm Math and PharmacologyRachel Cumbie KollenОценок пока нет
- Ocne 8 SupportДокумент9 страницOcne 8 Supportapi-349380871Оценок пока нет
- anesthesia records sДокумент5 страницanesthesia records sAnna Margarett MutiaОценок пока нет
- Carpal Tunnel Syndrome PowerPointДокумент15 страницCarpal Tunnel Syndrome PowerPointRadja DhilahОценок пока нет
- Ms 09: Burns: Curling's UlcerДокумент2 страницыMs 09: Burns: Curling's UlcerMary AgorillaОценок пока нет
- Abdo and HerniasДокумент6 страницAbdo and Herniasjoedeegan_Оценок пока нет
- Persiapan Triage Primary Survey Resusitasi Adjunct Primary: By: RiswanДокумент7 страницPersiapan Triage Primary Survey Resusitasi Adjunct Primary: By: Riswanrudi mirinoОценок пока нет
- Idoc - Pub - Critical Care Nursing Assessment FormДокумент3 страницыIdoc - Pub - Critical Care Nursing Assessment FormNamra AnsariОценок пока нет
- Goal #1-Patient Will ReportДокумент1 страницаGoal #1-Patient Will ReportRita Lala ElmerОценок пока нет
- Subjective: " " Sto: Diagnostics: Sto:Goal MET: VitalДокумент3 страницыSubjective: " " Sto: Diagnostics: Sto:Goal MET: VitalKarl KiwisОценок пока нет
- Medical TerminologyДокумент8 страницMedical Terminologyiannello100% (1)
- REEMP AND SHIPBOARD REME Form B v4 20200730Документ1 страницаREEMP AND SHIPBOARD REME Form B v4 20200730Click TechnologyОценок пока нет
- Echo ReportДокумент2 страницыEcho ReportweareweОценок пока нет
- Presentasi Code Blue IGDДокумент16 страницPresentasi Code Blue IGDIgd Pondok TjandraОценок пока нет
- Alternative Learning System Related Learning Experience Surgical WardДокумент13 страницAlternative Learning System Related Learning Experience Surgical WardRoshin TejeroОценок пока нет
- Brief RAM Assessment/Data Collection Sheet: DescriptionДокумент5 страницBrief RAM Assessment/Data Collection Sheet: DescriptionMary WanjiruОценок пока нет
- Hip FractureДокумент3 страницыHip Fracturenursing concept mapsОценок пока нет
- 189 Gotera, Chloe Lynn M. - Day 3Документ6 страниц189 Gotera, Chloe Lynn M. - Day 3Chloe GoteraОценок пока нет
- Patient Information: Location DateДокумент2 страницыPatient Information: Location DateGisselle PauloОценок пока нет
- Blood Transfusion Vsim Nursing WorksheetДокумент1 страницаBlood Transfusion Vsim Nursing Worksheetapi-688564858Оценок пока нет
- Acetylsalicilic Acid 500mg (Aspirin 500)Документ8 страницAcetylsalicilic Acid 500mg (Aspirin 500)asdwasdОценок пока нет
- Mental Health ResourcesДокумент5 страницMental Health ResourcesAnna R ZahorОценок пока нет
- NURS FPX 6618 Assessment 1 Planning and Presenting A Care Coordination ProjectДокумент5 страницNURS FPX 6618 Assessment 1 Planning and Presenting A Care Coordination ProjectEmma WatsonОценок пока нет
- Estradiol 1mg + Norethisterone Acetate 0.5mg (Activelle)Документ12 страницEstradiol 1mg + Norethisterone Acetate 0.5mg (Activelle)asdwasdОценок пока нет
- Two Step TSTДокумент2 страницыTwo Step TSTBrianHoОценок пока нет
- University of Caloocan City: Bachelor of Arts Major in Political Science The Problem and Its BackgroundДокумент7 страницUniversity of Caloocan City: Bachelor of Arts Major in Political Science The Problem and Its BackgroundJericko Perez AvilaОценок пока нет
- Dme Information Form Cms-10125 - External Infusion PumpsДокумент2 страницыDme Information Form Cms-10125 - External Infusion PumpsSonof GoddОценок пока нет
- Case Presentation OF Acute Tonsillitis: Nueva Ecija University of Science andДокумент38 страницCase Presentation OF Acute Tonsillitis: Nueva Ecija University of Science andBeverly DatuОценок пока нет
- A Materia Medica Comparison of Bowel Nosodes and Related Homoeopathic RemediesДокумент211 страницA Materia Medica Comparison of Bowel Nosodes and Related Homoeopathic RemediesjakОценок пока нет
- Nursing Care of Children with Physiologic and Hematologic DisordersДокумент17 страницNursing Care of Children with Physiologic and Hematologic DisordersDgjj CompuiterОценок пока нет
- CHMM Exam Blueprint Details Hazardous Materials Management Certification RequirementsДокумент2 страницыCHMM Exam Blueprint Details Hazardous Materials Management Certification RequirementswoowangsiОценок пока нет
- Nutritional Management of Short Bowel Syndrome PDFДокумент10 страницNutritional Management of Short Bowel Syndrome PDFSonya YunitaОценок пока нет
- Material Safety Data Sheet: Section 01: Product and Company IdentificationДокумент9 страницMaterial Safety Data Sheet: Section 01: Product and Company IdentificationMaya SeptianaОценок пока нет
- Block M2 EYE Distribution by MMCДокумент3 страницыBlock M2 EYE Distribution by MMCF ParikhОценок пока нет
- Monitoring Tool For Sped AДокумент3 страницыMonitoring Tool For Sped ARica Claire SerqueñaОценок пока нет
- Indian Herbs For Healthy Body - Healing Properties of Adalodakam, Arogya Pacha, Ashokam, IrattimadhuДокумент4 страницыIndian Herbs For Healthy Body - Healing Properties of Adalodakam, Arogya Pacha, Ashokam, IrattimadhuNEELОценок пока нет
- RA For SPT Test (Reviewed)Документ5 страницRA For SPT Test (Reviewed)shamshad ahamedОценок пока нет
- PAR-Q Physical Activity Readiness QuestionnaireДокумент3 страницыPAR-Q Physical Activity Readiness QuestionnaireMhervin BisisОценок пока нет
- Lupus and Pregnancy ComplicationsДокумент4 страницыLupus and Pregnancy ComplicationsDivika ShilvanaОценок пока нет
- What Is AmpalayaДокумент5 страницWhat Is Ampalayarugu0% (1)
- Physio Assess Form Oct 2022Документ5 страницPhysio Assess Form Oct 2022RishaadОценок пока нет
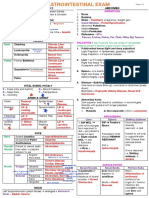
- Gastroenterology - Pancreatitis PDFДокумент2 страницыGastroenterology - Pancreatitis PDFMonica J Ortiz PereiraОценок пока нет
- Quiz2 1 Issue2Документ2 страницыQuiz2 1 Issue2Jazur AhamedОценок пока нет
- Holy Fire Reiki SymbolsДокумент3 страницыHoly Fire Reiki Symbolsharish.userОценок пока нет
- 272d0481-78d1 - US - SASOLAB 240 - EN-USДокумент9 страниц272d0481-78d1 - US - SASOLAB 240 - EN-USTania ZelayaОценок пока нет
- Legacy of Tuskegee Syphilis StudyДокумент2 страницыLegacy of Tuskegee Syphilis StudyLcgessamanОценок пока нет
- The New Jose L. Amante Emergency HospitalДокумент29 страницThe New Jose L. Amante Emergency HospitalRiah Ramirez FojasОценок пока нет
- Literature ReviewДокумент2 страницыLiterature ReviewKymani SutherlandОценок пока нет
- A Neurocognitive DisorderДокумент4 страницыA Neurocognitive Disordersitty upamОценок пока нет
- Paracetamol 10mg/ml Solution For Infusion PIL - UKДокумент2 страницыParacetamol 10mg/ml Solution For Infusion PIL - UKnurainiОценок пока нет