Вам также может понравиться
- ACO Final ReportДокумент24 страницыACO Final ReportSowmya ParthasarathyОценок пока нет
- RN MedSurgДокумент685 страницRN MedSurgArgyll Baye Ansuas100% (4)
- Textbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordОт EverandTextbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordОценок пока нет
- Management Analysis of HealthcareДокумент9 страницManagement Analysis of HealthcareMarshaPattersonОценок пока нет
- Ways To Improve The Health SystemДокумент18 страницWays To Improve The Health SystemB I N SОценок пока нет
- 5 Ways To Improve The Quality of HealthcareДокумент12 страниц5 Ways To Improve The Quality of Healthcarekasthu75Оценок пока нет
- Turning The Vision of Connected Health Into A RealityДокумент14 страницTurning The Vision of Connected Health Into A RealityCognizant100% (2)
- Group Practice Journal: Key Success Factors For Private Practice Hospital Medicine GroupsДокумент4 страницыGroup Practice Journal: Key Success Factors For Private Practice Hospital Medicine GroupsMhini Baba JayОценок пока нет
- Health Policy Brief: Accountable Care OrganizationsДокумент6 страницHealth Policy Brief: Accountable Care Organizationspalak32Оценок пока нет
- Data-Driven Healthcare Organizations Use Big Data Analytics For Big GainsДокумент8 страницData-Driven Healthcare Organizations Use Big Data Analytics For Big GainsHandsome RobОценок пока нет
- Myanmar Regulatory and Market ProfileДокумент15 страницMyanmar Regulatory and Market ProfileMaaz Khan100% (1)
- Glaxosmithkline Case SolutionДокумент5 страницGlaxosmithkline Case SolutionUmar Faruq EftiОценок пока нет
- Team Delivery Report PDFДокумент32 страницыTeam Delivery Report PDFwendyОценок пока нет
- The Best Laid Plans of Dogs and Vets: Transform Your Veterinary Practice Through Pet Health Care PlansОт EverandThe Best Laid Plans of Dogs and Vets: Transform Your Veterinary Practice Through Pet Health Care PlansОценок пока нет
- 4.strategy of The Bezos-Buffett-Dimon-Gawande Healthcare VentureДокумент7 страниц4.strategy of The Bezos-Buffett-Dimon-Gawande Healthcare VentureSai TejaОценок пока нет
- President & CEO: Message From TheДокумент7 страницPresident & CEO: Message From Theneyj_8Оценок пока нет
- The New Model of Primary Care: Reimbursement ScenariosДокумент13 страницThe New Model of Primary Care: Reimbursement ScenariosHeather WiemanОценок пока нет
- Comparative Health Information Management 4th Edition Peden Solutions Manual 1Документ13 страницComparative Health Information Management 4th Edition Peden Solutions Manual 1daisy100% (32)
- Family Care Specialists Medical Group, Inc. Acct 521 Group Members: Garrett Pfeiffer, Jacob Kang, Ploy Wongthavarawat, Shami MadakshiraДокумент3 страницыFamily Care Specialists Medical Group, Inc. Acct 521 Group Members: Garrett Pfeiffer, Jacob Kang, Ploy Wongthavarawat, Shami MadakshiraBecky WangОценок пока нет
- Identifying and Resolving Disputes in New Accountable Care SettingsДокумент10 страницIdentifying and Resolving Disputes in New Accountable Care SettingsRothHealthLawОценок пока нет
- Managing The Health Benefits Supply ChainДокумент12 страницManaging The Health Benefits Supply ChainJim RoseОценок пока нет
- American Wells Case SolutionДокумент3 страницыAmerican Wells Case SolutionAnne SinitraОценок пока нет
- 40 A National Strategy Pp982 990Документ9 страниц40 A National Strategy Pp982 990cma909Оценок пока нет
- Hospital CEO Best Practices: A Ab BSST TR Ra Ac CT TДокумент6 страницHospital CEO Best Practices: A Ab BSST TR Ra Ac CT Tfrancisco_expósitoОценок пока нет
- Managed Healthcare: Industry OverviewДокумент11 страницManaged Healthcare: Industry Overviewt6166asОценок пока нет
- Technical and Allocative Efficiency in The HospitalДокумент9 страницTechnical and Allocative Efficiency in The HospitalShubham AgarwalОценок пока нет
- 2020 Health Benefit Summary PDFДокумент36 страниц2020 Health Benefit Summary PDFTitoОценок пока нет
- Executive Perspectives: Hsas More Effective at Consumer Engagement Than HrasДокумент4 страницыExecutive Perspectives: Hsas More Effective at Consumer Engagement Than HrasAutomotive Wholesalers Association of New EnglandОценок пока нет
- Assignment TasksДокумент4 страницыAssignment TasksMuhammad Faraz HasanОценок пока нет
- Marketing Management - 1 Assignment: Group 10Документ4 страницыMarketing Management - 1 Assignment: Group 10m3gp13 yoОценок пока нет
- HW5Документ4 страницыHW5Karthik GanesuniОценок пока нет
- Billing Service: What To Look For When Selecting A Billing ServiceДокумент7 страницBilling Service: What To Look For When Selecting A Billing ServicezahidmОценок пока нет
- Payers & Providers National Edition - Issue of July 2012Документ8 страницPayers & Providers National Edition - Issue of July 2012PayersandProvidersОценок пока нет
- Using Behavioral Science To Improve The Customer Experience: February 2010Документ5 страницUsing Behavioral Science To Improve The Customer Experience: February 2010Ankush SharmaОценок пока нет
- Research Paper Employee BenefitsДокумент7 страницResearch Paper Employee Benefitspdtgpuplg100% (1)
- PhysicianДокумент16 страницPhysicianHaru RodriguezОценок пока нет
- MIS AssignmentДокумент3 страницыMIS AssignmentMOHAMAD FERDIANSYAH ARIFIN BIN OMER SA'AIB STUDENTОценок пока нет
- Cost Reduction Strategies For Health SystemsДокумент6 страницCost Reduction Strategies For Health SystemsBruhan Kaggwa100% (1)
- HCD WP 2012 ValueBasedPurchasingWhatHospitalsAndHealthSystemsNeedДокумент8 страницHCD WP 2012 ValueBasedPurchasingWhatHospitalsAndHealthSystemsNeedPatBickleyОценок пока нет
- A - 6 - American WellДокумент4 страницыA - 6 - American WellRupam ChakrabortyОценок пока нет
- Exercise Pros Action Guide Clickable LinksДокумент9 страницExercise Pros Action Guide Clickable LinksbalialkoushikОценок пока нет
- Developing Organizational Policies and Practices AДокумент7 страницDeveloping Organizational Policies and Practices Amutisya johnboscoОценок пока нет
- Auc 5Документ6 страницAuc 5safОценок пока нет
- Hospital Management Research PapersДокумент8 страницHospital Management Research Papersaflbsybmc100% (1)
- WP Insight HCR Impact On Rewards StrategiesДокумент4 страницыWP Insight HCR Impact On Rewards StrategiesGeorge B. BuckОценок пока нет
- Chapter 5 - Provider Reimbursement MethodsДокумент18 страницChapter 5 - Provider Reimbursement MethodsAdityaОценок пока нет
- Ahm 250Документ91 страницаAhm 250hemanthtikyani100% (1)
- Issues: Accreditation HippaДокумент61 страницаIssues: Accreditation HippajevetteОценок пока нет
- What Do Employer's Want For Their Employees?: Standardization With IndividualizationДокумент4 страницыWhat Do Employer's Want For Their Employees?: Standardization With Individualizationapi-304631562Оценок пока нет
- What Do Employer's Want For Their Employees?: Standardization With IndividualizationДокумент4 страницыWhat Do Employer's Want For Their Employees?: Standardization With Individualizationapi-304631562Оценок пока нет
- Healthcare Financial Management DiscussionsДокумент17 страницHealthcare Financial Management Discussionsapi-655123959Оценок пока нет
- 8973308Документ9 страниц8973308Anonymous mWI4Hktm50% (2)
- Employee Health InvestmentsДокумент5 страницEmployee Health InvestmentsAnuОценок пока нет
- Paying For Quality CaseДокумент14 страницPaying For Quality CaseWILFRED ZVAREVASHEОценок пока нет
- Final Project For HINT 220Документ16 страницFinal Project For HINT 220Maxine WhiteОценок пока нет
- HPN6Документ50 страницHPN6Joy MichaelОценок пока нет
- Payment in Healthcare OrganizationsДокумент12 страницPayment in Healthcare Organizationsevans kirimiОценок пока нет
- How To Avoid Conflicts Between Your New EHR and Your Old Billing CompanyДокумент5 страницHow To Avoid Conflicts Between Your New EHR and Your Old Billing CompanyM. SmithОценок пока нет
- Pharmacists in Health Care Management TranscriptДокумент8 страницPharmacists in Health Care Management TranscriptrakutenmeeshoОценок пока нет
- Starting New Job ChecklistДокумент2 страницыStarting New Job ChecklistSalsabeel ArshadОценок пока нет
- Case 2 TelemonitoringДокумент5 страницCase 2 Telemonitoringapi-300829020Оценок пока нет
- Health Economics Note Chapter 12Документ12 страницHealth Economics Note Chapter 12Farian Tahrim VikiОценок пока нет
- Cancer of Unknown PrimaryДокумент12 страницCancer of Unknown Primaryraul gutierrezОценок пока нет
- Delirium in The Intensive Care Unit Is Dexmedetomidine EffectiveДокумент15 страницDelirium in The Intensive Care Unit Is Dexmedetomidine EffectiveArgenis SalinasОценок пока нет
- Activity 1Документ2 страницыActivity 1cherrielОценок пока нет
- 5 3672 Ivica IvekovicДокумент41 страница5 3672 Ivica IvekovicplavaadresaОценок пока нет
- Oswestry Disability Index (ODI)Документ3 страницыOswestry Disability Index (ODI)Mohamed ZakiОценок пока нет
- Segurança e Tax de Lesoes PDFДокумент20 страницSegurança e Tax de Lesoes PDFFilipeAssunçãoОценок пока нет
- Soal PAS BIG Xi, SMT 3, OnlineДокумент10 страницSoal PAS BIG Xi, SMT 3, OnlineRivaldi Lukman HakimОценок пока нет
- Representations of Personalised Medicine in Family HealthДокумент9 страницRepresentations of Personalised Medicine in Family HealthAbCcОценок пока нет
- Borrescio-Higa Valenzuela - Gender Inequality and Mental Health.Документ9 страницBorrescio-Higa Valenzuela - Gender Inequality and Mental Health.Firdaus Silabi Al-AttarОценок пока нет
- Mentor Interview Questions TemplateДокумент3 страницыMentor Interview Questions Templateapi-381640393Оценок пока нет
- 7724 (11) The Hospital and Pertinent Laws and RegulationsДокумент24 страницы7724 (11) The Hospital and Pertinent Laws and RegulationsnewazОценок пока нет
- Tutor: Dr. Vera Dr. Haerani: Skenario Problems Learning Objectives Main Map ReferensiДокумент36 страницTutor: Dr. Vera Dr. Haerani: Skenario Problems Learning Objectives Main Map ReferensiAdeLia Nur FitrianaОценок пока нет
- Cognition, Cognitive Rehabilitation, and Occupational PerformanceДокумент23 страницыCognition, Cognitive Rehabilitation, and Occupational PerformanceMaria AiramОценок пока нет
- Food Industry Project PDFДокумент21 страницаFood Industry Project PDFMahraf Mohammad 2012353630Оценок пока нет
- Do's and Dont's in Writing Research QuestionsДокумент2 страницыDo's and Dont's in Writing Research QuestionsLisandrea BrownОценок пока нет
- VSO Our Side of The Story Uganda - Full ReportДокумент68 страницVSO Our Side of The Story Uganda - Full ReportVSOОценок пока нет
- Hussen Worku 2022 Quality of Antenatal Care Service and Factors Associated With Client Satisfaction at Public HealthДокумент9 страницHussen Worku 2022 Quality of Antenatal Care Service and Factors Associated With Client Satisfaction at Public HealthEkung EmmanuelОценок пока нет
- Reviewer in English 5Документ2 страницыReviewer in English 5Christine HernandezОценок пока нет
- MCN Lec M1L1 ReviewerДокумент4 страницыMCN Lec M1L1 ReviewerEmily BernatОценок пока нет
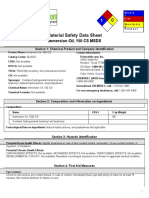
- 0 Material Safety Data Sheet: Immersion Oil, 150 CS MSDSДокумент5 страниц0 Material Safety Data Sheet: Immersion Oil, 150 CS MSDSA.N. MОценок пока нет
- A2 1021V en Bowen w7Документ47 страницA2 1021V en Bowen w7Gareth GriffithsОценок пока нет
- Titanium IV OxideДокумент8 страницTitanium IV OxideFransiscus Xaverius Patrick RustanОценок пока нет
- PMFIAS CA 2019 05 12 SciДокумент107 страницPMFIAS CA 2019 05 12 SciShivy SwarnkarОценок пока нет
- VAW ToT Caribbean May 2019 DAY 1Документ77 страницVAW ToT Caribbean May 2019 DAY 1NITU SHARMAОценок пока нет
- Jurisprudence Direct Exam of Expert WitnessДокумент9 страницJurisprudence Direct Exam of Expert WitnessxquisiteDОценок пока нет
- All India Institute of Medical Sciences, New Delhi-110 029 (Examination Section)Документ1 страницаAll India Institute of Medical Sciences, New Delhi-110 029 (Examination Section)Nitin SinghalОценок пока нет
- Disaster Nursing Lecture 1Документ11 страницDisaster Nursing Lecture 1Beahtriz GuintoОценок пока нет
- A 6 Phlebitis and Infiltration ScalesДокумент1 страницаA 6 Phlebitis and Infiltration ScalesSorin Alexandru LucaОценок пока нет