Вам также может понравиться
- Young Adult BrochureДокумент5 страницYoung Adult BrochureahsanОценок пока нет
- Benefit Highlights: AARP Medicare Advantage Choice (PPO)Документ3 страницыBenefit Highlights: AARP Medicare Advantage Choice (PPO)EstherОценок пока нет
- Choice MVДокумент1 страницаChoice MVGowell SupportОценок пока нет
- Your Customized Benefits Plan at HCL America IncДокумент2 страницыYour Customized Benefits Plan at HCL America IncShiv RanjanОценок пока нет
- Eb 2019 Oe Guideplussbc GenericДокумент19 страницEb 2019 Oe Guideplussbc GenericCybernaughtОценок пока нет
- Protect What You Treasure Most: HealthДокумент12 страницProtect What You Treasure Most: HealthNelly HОценок пока нет
- 2020 Health Benefits Table PDFДокумент1 страница2020 Health Benefits Table PDFTitoОценок пока нет
- Kaiser Permanente California Plans and Benefits Brochure KPIF 2011Документ6 страницKaiser Permanente California Plans and Benefits Brochure KPIF 2011DennisОценок пока нет
- Pet Insurance ComparisonsДокумент2 страницыPet Insurance ComparisonsHSVC50% (2)
- IncomeShield Standard Plan benefits at a glanceДокумент18 страницIncomeShield Standard Plan benefits at a glanceHihiОценок пока нет
- Core MVДокумент1 страницаCore MVGowell SupportОценок пока нет
- Benefits Highlights 2018Документ5 страницBenefits Highlights 2018Marcus CosmeОценок пока нет
- Income Incomeshield Contract With Schedule v202304Документ20 страницIncome Incomeshield Contract With Schedule v202304Harry SmithОценок пока нет
- First Help PlanДокумент1 страницаFirst Help PlanIvan QuevedoОценок пока нет
- An Extras Cover For A Healthier LifestyleДокумент6 страницAn Extras Cover For A Healthier LifestylealterchicОценок пока нет
- CHI - One Pager - Version 1.3 - September 2021Документ1 страницаCHI - One Pager - Version 1.3 - September 2021ShihbОценок пока нет
- Kaiser Permanente Compare Plans CA 2011 KPIFДокумент1 страницаKaiser Permanente Compare Plans CA 2011 KPIFDennis AlexanderОценок пока нет
- 2019 Plan BenefitsДокумент14 страниц2019 Plan BenefitsMichelleJeungОценок пока нет
- A In-Hospital Care: INTEGRATED GHSMM Insurance PlanДокумент1 страницаA In-Hospital Care: INTEGRATED GHSMM Insurance PlanMOHAMAD SHAWALОценок пока нет
- Brochure - EZCare (Nov 2022)Документ11 страницBrochure - EZCare (Nov 2022)Darren ChenОценок пока нет
- 2010 UHC Medical Plan ComparisonДокумент2 страницы2010 UHC Medical Plan Comparisonapi-20618861Оценок пока нет
- Benefit at A GlanceДокумент2 страницыBenefit at A GlanceShiv ChauhanОценок пока нет
- Services Marketing "Shouldice Hospital Limited" - Case SubmissionДокумент6 страницServices Marketing "Shouldice Hospital Limited" - Case SubmissionVenkata Sai Pavan JeerlaОценок пока нет
- Summary of 2022 Benefit Changes: MedicalДокумент5 страницSummary of 2022 Benefit Changes: MedicalChinnu SalimathОценок пока нет
- RetrieveCustomBrochure (OMAR GAAFAR MOHAMMED SAIF BAGGASH)Документ3 страницыRetrieveCustomBrochure (OMAR GAAFAR MOHAMMED SAIF BAGGASH)Omar BaggashОценок пока нет
- Unitedhealthcare Dental Hmo Plan 2022 Summary of Benefits and CoverageДокумент9 страницUnitedhealthcare Dental Hmo Plan 2022 Summary of Benefits and CoverageAdam CliftonОценок пока нет
- Keystone HMO Gold Preferred 4080650Документ11 страницKeystone HMO Gold Preferred 4080650ANKIT SINGHОценок пока нет
- Compass: Gold / SilverДокумент16 страницCompass: Gold / SilverStan SmithОценок пока нет
- CHI One PagerДокумент1 страницаCHI One PagerPOS-ADSR TrackingОценок пока нет
- ReyForBusiness (Group) - Plan & Price Sampling - 2023Документ7 страницReyForBusiness (Group) - Plan & Price Sampling - 2023Nadhifah Nur HafshahОценок пока нет
- Barbados NemCare Individuals Health InsuranceДокумент3 страницыBarbados NemCare Individuals Health InsuranceKammieОценок пока нет
- EQ Employee Benefits Plan Brochure (January 2023)Документ8 страницEQ Employee Benefits Plan Brochure (January 2023)Darren ChenОценок пока нет
- 2022 Steven Charles BAG - COДокумент4 страницы2022 Steven Charles BAG - COAlejuanchis Kamacho GarciaОценок пока нет
- Manulife CoverMe FollowMe Health Comp Chart Jan 2018 ENGLISHДокумент2 страницыManulife CoverMe FollowMe Health Comp Chart Jan 2018 ENGLISHMamacintОценок пока нет
- The Essential Plan Chart WnyДокумент1 страницаThe Essential Plan Chart WnyJavier GramajoОценок пока нет
- Bariatric GuideДокумент20 страницBariatric GuideMuhammad Hadi AkbarОценок пока нет
- International Travel Insurance - Future GeneraliДокумент6 страницInternational Travel Insurance - Future GeneraliRizwan KhanОценок пока нет
- Generic Open Enrollment KitДокумент22 страницыGeneric Open Enrollment KitSteve BarrowsОценок пока нет
- 2010 UnitedHealthcare Benefits SummaryДокумент1 страница2010 UnitedHealthcare Benefits Summaryapi-27017317Оценок пока нет
- VOYA USG Accident-Hospital IndemnityДокумент37 страницVOYA USG Accident-Hospital IndemnityDavid BriggsОценок пока нет
- GlobalCare Health Plan Benefits at a GlanceДокумент7 страницGlobalCare Health Plan Benefits at a GlanceIrwanto AyongОценок пока нет
- Cardea Schedule of Benefits Effective Jan 1st 2021Документ4 страницыCardea Schedule of Benefits Effective Jan 1st 2021Wayne GajadharОценок пока нет
- 44 Bed Detox and Residential Substance Abuse Treatment Facility Proforma - Chapman TustinДокумент4 страницы44 Bed Detox and Residential Substance Abuse Treatment Facility Proforma - Chapman TustinDaniel L. Case, Sr.100% (2)
- Property & Liability Renewal ComparisonДокумент58 страницProperty & Liability Renewal Comparisonpalanisamy744100% (1)
- EmblemHealth Benefits 2019Документ7 страницEmblemHealth Benefits 2019Jorge Luis Rivera AgostoОценок пока нет
- Your guide to 70% back on included extras with black 70 boostДокумент6 страницYour guide to 70% back on included extras with black 70 boostSaifuddin SidikiОценок пока нет
- Summary of Benefits: Silver Trio Hmo 2300/70 OffexДокумент12 страницSummary of Benefits: Silver Trio Hmo 2300/70 OffexjaroopaitummaiОценок пока нет
- HCOs Variances SolДокумент3 страницыHCOs Variances SolSimon OllyОценок пока нет
- Income FlexCareДокумент22 страницыIncome FlexCareDarren ChenОценок пока нет
- Fhpv23apr231218j7r2 Veasna UkДокумент6 страницFhpv23apr231218j7r2 Veasna UkSela SinОценок пока нет
- Manu 3Документ4 страницыManu 3Temp RoryОценок пока нет
- Cash Plan 100 Table+of+coverДокумент8 страницCash Plan 100 Table+of+covermuthukumaran.tdr2969Оценок пока нет
- A plan for every health needДокумент8 страницA plan for every health needgouravbhatia200189Оценок пока нет
- GSH GTC Benefit Schedule and Premium RatesДокумент19 страницGSH GTC Benefit Schedule and Premium RatesChin Mui LanОценок пока нет
- 2018 Mhealth DirectДокумент2 страницы2018 Mhealth DirectSasha NelsonОценок пока нет
- Análise Custo Beneficio DESДокумент21 страницаAnálise Custo Beneficio DESRui FonteОценок пока нет
- Blue ChoiceДокумент5 страницBlue ChoiceahsanОценок пока нет
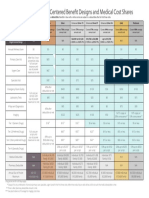
- Medical Comparison Chart 2020Документ3 страницыMedical Comparison Chart 2020hollingermikeОценок пока нет
- Snap Guardian Dental Plan Summary 2022Документ4 страницыSnap Guardian Dental Plan Summary 2022Samson FungОценок пока нет
- Ask Assess Advise ExplainedДокумент1 страницаAsk Assess Advise Explainedlanamalay12100% (1)
- CFR 2010 Title21 Vol4 ChapIДокумент197 страницCFR 2010 Title21 Vol4 ChapIMohamed ZhranОценок пока нет
- SH Conversation ExampleДокумент2 страницыSH Conversation ExampleHannah WilkerОценок пока нет
- Second PrescriptionДокумент6 страницSecond Prescriptionssuhass243Оценок пока нет
- Healthcare - Gov/sbc-Glossary: Important Questions Answers Why This MattersДокумент8 страницHealthcare - Gov/sbc-Glossary: Important Questions Answers Why This Mattersapi-252555369Оценок пока нет
- Vii Eng Second Mid Term Online Exam QuestionДокумент5 страницVii Eng Second Mid Term Online Exam QuestionAsghar AliОценок пока нет
- Prescription Reimb Claim FormДокумент2 страницыPrescription Reimb Claim FormimthedciОценок пока нет
- Patient Satisfaction With Healthcare Services: A Bangladesh ScenarioДокумент8 страницPatient Satisfaction With Healthcare Services: A Bangladesh ScenarioA. K. MohiuddinОценок пока нет
- Test Bank For Roachs Introductory Clinical Pharmacology 11th Edition Susan M FordДокумент9 страницTest Bank For Roachs Introductory Clinical Pharmacology 11th Edition Susan M FordJack WittersОценок пока нет
- Top 10 medication safety tips and reducing high-risk medication errorsДокумент1 страницаTop 10 medication safety tips and reducing high-risk medication errorsGabee MoralesОценок пока нет
- National Quality Assurance Program Updates: Standards, Awards and InitiativesДокумент48 страницNational Quality Assurance Program Updates: Standards, Awards and InitiativessourabhОценок пока нет
- 150Документ68 страниц150Andrei Miguel RoqueОценок пока нет
- Project Scope StatementДокумент4 страницыProject Scope StatementAndreosPapadopoloCruz50% (2)
- Law and EthicsДокумент11 страницLaw and EthicslkvhqjsgdОценок пока нет
- Policy On Generic Prescribing and RecordingДокумент19 страницPolicy On Generic Prescribing and RecordingagelesswapОценок пока нет
- Tata 1mg Return & Refund Policy SummaryДокумент5 страницTata 1mg Return & Refund Policy Summarys m sufiyanОценок пока нет
- Compendium On Drug Education 1Документ194 страницыCompendium On Drug Education 1Lombroso's followerОценок пока нет
- 2017 Anthem GHIP Benefits Booklet (Final)Документ119 страниц2017 Anthem GHIP Benefits Booklet (Final)Alexander NewberryОценок пока нет
- Poster PresentationДокумент1 страницаPoster PresentationsjОценок пока нет
- Prohibited Acts and Penalties under the Dangerous Drugs ActДокумент6 страницProhibited Acts and Penalties under the Dangerous Drugs ActRobert Vincent Astudillo Angeles IVОценок пока нет
- Fundamentals of Pharmacology Australian 7th Edition Bullock Test BankДокумент7 страницFundamentals of Pharmacology Australian 7th Edition Bullock Test BankJamesFrancisrwnmi100% (16)
- ER-Diagram ExplanationsДокумент3 страницыER-Diagram ExplanationsGokay GulsoyОценок пока нет
- Delos Santos v. CoAДокумент2 страницыDelos Santos v. CoARonnie RimandoОценок пока нет
- PMP NextGen SoftwareДокумент16 страницPMP NextGen SoftwareHussam MomaniОценок пока нет
- Medication History InterviewДокумент2 страницыMedication History InterviewShaik SameenaОценок пока нет
- Zest Pharma, MarketingДокумент6 страницZest Pharma, Marketingbhawsar_indore100% (1)
- Gilead FCA LawsuitДокумент68 страницGilead FCA LawsuitAlex Kacik100% (5)
- MP Pakistan Q1 2016Документ102 страницыMP Pakistan Q1 2016Ahmed AshrafОценок пока нет
- Computer Application in Pharmacy HK Technical PGIMSДокумент14 страницComputer Application in Pharmacy HK Technical PGIMSsjОценок пока нет
- California 3 Tier Drug ListДокумент156 страницCalifornia 3 Tier Drug ListSangram KhandareОценок пока нет