Академический Документы
Профессиональный Документы
Культура Документы
Brain Death & Organ Procurement
Загружено:
kencheenИсходное описание:
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Brain Death & Organ Procurement
Загружено:
kencheenАвторское право:
Доступные форматы
3.
5 HOURS
Continuing Education
By Kathleen M. Z. Peiffer, BSN, RN, CCRN
Brain Death and
Organ Procurement
Nursing management of adults with brain injury is crucial
to the viability of donor organs.
of Health and Human Services and hospital and
transplantation leaders recently formed the Organ
Overview: Patients with severe brain injuries (as can result from Donation Breakthrough Collaborative. Between
trauma, subarachnoid hemorrhage, or brain tumor) are moni- 2003 and 2005, the organ donation rate rose 18%;
tored closely by nursing staff. It’s often the nurse who first recog- but it’s still far short of what experts believe is
possible.2
nizes clinical signs of decompensation and begins the process of Clinicians bear part of the responsibility for this.
determining whether the patient is a potential organ donor. If interventions after brain death are not aggressive
When a person is declared brain dead, it’s the nurse who main- and timely, the body’s tissues and organs cannot be
tains hemodynamic stability so that donor organs remain viable. used for transplantation. Indeed, when a patient is a
potential or designated organ donor, the nursing
It’s therefore crucial for nurses to know how brain death is deter- care required may be even more rigorous after brain
mined in adults and how potential organ donors are identified, death than before. (At my facility, the nurse–patient
and to know the major physiologic changes that occur upon ratio for brain-dead organ donors may be as high as
3:1.) Consider this: one organ donor can provide as
brain death, as well as essential nursing interventions.
many as 50 different organs and tissues to recipi-
ents.3 Yet although essential to the successful recov-
ery and long-term survival of viable organs,4 donor
management is considered “one of the most neglected
T
he need for donor organs far outstrips areas of transplantation.”5
their availability. More than 94,000 The transition from caring for the living to caring
people nationwide are on waiting lists for the brain dead (as potential organ donors) can
for organs, yet from January through be difficult for nurses. How does your role change
September 2006, just 22,014 transplan- when you begin working with a brain-dead patient
tations were performed, according to the United and an organ-procurement coordinator?
Network for Organ Sharing (UNOS).1 Until recently,
the donation rate among potential donors was less IDENTIFYING ORGAN DONORS: THE NURSE’S JOB
than 50%: of 14,000 potential donors identified in Patients with severe brain injuries (as can result
2002, fewer than half (46%) donated organs.2 In an from trauma, subarachnoid hemorrhage, or brain
effort to improve that rate, the U.S. Department tumor) are monitored closely by nursing staff. It’s
therefore often the nurse who first recognizes signs
Kathleen M. Z. Peiffer is a student in the master’s program in
of decompensation (such as a lack of eye, verbal,
nurse anesthesia in the College of Nursing and Health and motor responses according to the Glasgow
Professions at Drexel University, Philadelphia, and a per diem Coma Scale and the absence of ventilatory
nurse in the surgical ICU at Holy Spirit Hospital, Camp Hill, attempts) and begins the process of determining
PA. Contact author: kzpeiffer@msn.com. The author of this
article has no significant ties, financial or otherwise, to any whether the patient is a potential organ donor.
company that might have an interest in the publication of this Indeed, frequent neurologic assessments to evaluate
educational activity. for signs of decompensation should be made before
58 AJN ▼ March 2007 ▼ Vol. 107, No. 3 http://www.nursingcenter.com
a
ho
B
Oc
lisa
ne
An
by
A
s
ion
trat
Illus
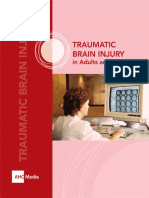
A) Subdural hematoma in the frontal lobe (not a cross-section; only skull has been removed)
B) Cross-section showing resulting brain swelling and herniation through the foramen magnum
a diagnosis of brain death, in order to protect tissue this can happen either when brain death is immi-
and organ viability. (See Determining Brain Death, nent or after it has been declared. (If the patient has
page 60.) just been declared brain dead, it’s important to give
Typically, the nurse first informs the attending the family time to understand the diagnosis and to
physician, the neurologist, or the neurosurgeon of absorb their loss before the prospect of organ dona-
the patient’s decompensation. Depending on the tion is discussed. The length of time needed will
facility’s protocol, either the nurse or another clini- vary from case to case.)
cian may then contact the local organ-procurement Once the attending physician has declared the
organization (OPO) to say that there is a case that time of brain death, the local OPO coordinator—
may soon involve them. Ideally, the local OPO who is often a nurse or physician assistant19—
should be contacted when brain death is imminent, assumes responsibility for the donor’s management,
before a declaration of brain death has been made.25 which includes directing clinical nursing care. The
However, if the OPO hasn’t been notified, that is OPO coordinator will direct the nursing staff to
done once brain death is declared. (For more on maintain hemodynamic stability of the body while
the history and responsibilities of OPOs, see Organ- the family reaches a decision about organ donation.
Procurement Organizations, page 63.) If the family opts for donation, the OPO coordina-
When brain death appears imminent, if not sooner, tor continues to direct care until the organs and tis-
the physician will inform the family of the severity of sues are released to representatives of the designated
the patient’s condition, and nurses will provide addi- recipients’ facilities.
tional support and information, as will clergy and The OPO coordinator typically leads the discus-
social workers. Either the physician or the OPO coor- sion about organ donation with a potential donor’s
dinator may bring up the subject of organ donation; family, with staff nurses providing emotional sup-
ajn@wolterskluwer.com AJN ▼ March 2007 ▼ Vol. 107, No. 3 59
Determining Brain Death
I n 1968, recognizing that advances in cardiopulmonary
resuscitation and life support were keeping hearts beat-
ing even when catastrophic brain damage had occurred,
the Ad Hoc Committee of the Harvard Medical School set
forth a new definition of death: irreversible coma.6 The
three primary criteria for diagnosis were total “unreceptiv-
ity and unresponsivity” to external stimuli, a complete lack
of spontaneous muscular movement or respiration, and
“the absence of elicitable reflexes.” A fourth, confirmatory
criterion—an isoelectric (flat) electroencephalogram
(EEG)—was also named. With some refinements, these
criteria have remained the standard. 1a
In 1981 a group of medical consultants to the
President’s Commission for the Study of Ethical Problems in 1b
Medicine and Biomedical and Behavioral Research pub-
lished Guidelines for the Determination of Death, which
clarified the need to confirm both the cessation of all brain organ hypoperfusion.17, 20 Although opinions vary as to the
function and the irreversibility of that condition, and speci- cause, some studies attribute the second collapse to a sec-
fied that drug intoxication, hypothermia, and shock must ond catecholamine release.17, 21
be ruled out.7 (This was the basis for the Uniform Confirmatory findings on neurologic assessment. In
Determination of Death Act of 1981, a model statute cases of imminent or suspected brain death, neurologic
intended to lessen legal “confusion”8; brain death legisla- assessment includes evaluating the level of coma or un-
tion has since been enacted in all 50 states.9) More responsiveness, testing brain stem reflexes, and assessing
recently, in 1994 the American Academy of Neurology for apnea.13, 22 The following findings, which are also out-
(AAN) defined brain death as “the absence of clinical lined in Brain Death: Confirmatory Findings on
brain function when the proximate cause is known and Neurologic Assessment, page 65, confirm brain death
demonstrably irreversible,” summarized practice parame- except in cases of hypothermia, drug intoxication, or con-
ters for determining its occurrence in adults, and discussed founding conditions such as acute metabolic or endocrine
specific tools and confirmatory tests.10 disturbances, all of which may be reversible.13, 22
When brain death occurs. Approximately 1% of all Level of coma or unresponsiveness. Although not all
deaths occur first in the brain rather than in the cardiopul- patients who are comatose progress to brain death, peo-
monary system, according to one expert.11 The most com- ple who are brain dead will be unresponsive to verbal
mon causes of brain death in adults are trauma and and painful stimuli. The Glasgow Coma Scale tests the lev-
subarachnoid hemorrhage, according to reviews12, 13; other els of verbal response to spoken stimuli (such as the
causes include infection such as meningitis or encephalitis patient’s name) and eye and motor response to both spo-
and brain tumor. ken and painful stimuli (such as pressure applied to the
The initial trauma sets off a cascade of events. 14-19 Tissue supraorbital nerve [1a] or nail beds [1b]). Total scores
damage and fluid blockage or excessive fluid accumulation ranging from 3 (lowest) to 15 (highest) are possible. A
result in increasing intracranial pressure, ischemia, and score of 3 indicates profound unresponsiveness.
brain cell death. When ischemia reaches the brain stem, it Respiratory findings. Normal respiration occurs when
triggers a massive release of catecholamines—an event the respiratory center of the brain (an area within the
known as an autonomic or sympathetic “storm”—which medulla oblongata and the pons) responds to rising serum
leads to an immediate, intense Cushing response (increased carbon dioxide levels. In a healthy brain, a partial pres-
systemic vascular resistance and hypertension) lasting about sure of carbon dioxide (PaCO2) level above 60 mmHg
15 minutes. Compression of the vasculature and worsening prompts respiration. In a patient who is brain dead, this
ischemia cause infarction of brain tissue. Venous engorge- response is absent.
ment and brain swelling cause the brain to herniate through To test for central apnea, the patient is taken off
the foramen magnum, further inhibiting cerebral perfusion. mechanical ventilation and 100% oxygen 6 L/min is deliv-
Inflammation and edema progress and intracranial pressure ered by nasal cannula for as long as eight minutes while
rises even more, culminating in a complete loss of cerebral the patient is observed for signs of attempted breathing.22
blood flow. An arterial blood gas sample is also obtained and the
As the sympathetic storm subsides, the initial Cushing PaCO2 level measured to ensure that carbon dioxide lev-
response is followed by a brief period of stability. Then a els are adequate to trigger respiration; if a PaCO2 level
second hemodynamic collapse occurs.17 This collapse is greater than 60 mmHg and no signs of attempted breath-
characterized by a profound loss of vascular tone and a ing are observed, the apnea test is confirmatory.
subsequent loss of peripheral resistance, bradycardia, Ocular reflex findings. The pupillary reflex is tested by
hypotension, plummeting cardiac output, and systemic shining a light into the patient’s eyes (2); normally the pupils
60 AJN ▼ March 2007 ▼ Vol. 107, No. 3 http://www.nursingcenter.com
2 3
5 6
constrict. If the pupils remain fixed and dilated at a size confirmatory (6). The gag reflex can be assessed either by
greater than 4 mm, this is confirmatory of brain death manually manipulating the endotracheal tube or by touch-
(except in cases of preexisting pupillary abnormalities).22 The ing a cotton-tipped applicator to the posterior pharynx,
oculovestibular test involves injecting about 10 mL of ice although as one article states, “the results can be difficult
water or saline into the ear canal (3). Ordinarily the patient’s to evaluate in orally intubated patients.”22
eyes will turn toward the stimulated ear. If no eye movement Confirmatory laboratory tests are optional in diagnos-
occurs, this test is confirmatory. In the oculocephalic test (also ing brain death in adults. However, the AAN recommends
known as the “doll’s eyes” test), the clinician moves the such tests “in patients in whom specific components of clini-
patient’s head from midline to each side in turn (4). Normally cal testing cannot be reliably performed or evaluated,”
the patient’s gaze remains on a specific point, with the eyes such as those with severe facial trauma.10 According to the
moving away from the direction of the head turn in order to AAN, the most sensitive test is cerebral angiography, but
maintain that gaze. In patients without this reflex, the eyes the contrast dye used can render organs useless for trans-
remain fixed at midline despite head movement. plantation. With patients who are potential or designated
Other reflexes. The corneal reflex is tested by gently organ donors, electroencephalography or cerebral scintig-
touching a sterile, cotton-tipped swab to the patient’s raphy is preferred. If the patient is brain dead, an EEG will
cornea and observing for a reaction (blinking or eye move- reveal an isoelectric pattern. Cerebral scintigraphy may be
ment [5]). Although the corneal reflex may be blunted nor- performed to verify the absence of cerebral blood flow23, 24;
mally (for example, in contact-lens wearers), it will be its advantages are that it can be performed at bedside and
absent in correlation with other assessment findings in does not pose a threat to organs.23 Other confirmatory tests
someone who is brain dead. The cough reflex may be may include transcranial Doppler ultrasonography and
tested by performing deep bronchial suctioning through somatosensory evoked potentials (responses evoked by
the patient’s endotracheal tube; a lack of response is electrical stimulation of peripheral nerves).
ajn@wolterskluwer.com AJN ▼ March 2007 ▼ Vol. 107, No. 3 61
port. Many people identify themselves as organ
donors on their driver’s license. Because that infor- Brain Death Criteria
mation can be useful in discussing the patient’s
wishes, the coordinator often contacts the state’s 1. Condition has a known cause.
department of motor vehicles before approaching 2. Condition is irreversible.
the family, to determine whether the patient has des- 3. Neuromuscular blocking agents and central
ignated herself or himself a donor. However, in most nervous system depressants are absent.
states it’s the family that makes the final determi- 4. Temperature is higher than 35°C (95°F).
nation. (For more on state regulations, see www. 5. Patient is apneic.
donatelife.net.) 6. Patient is areflexic.
The OPO coordinator is responsible for docu- Ad Hoc Committee of the Harvard Medical School to Examine the
Definition of Brain Death. JAMA 1968;205(6):337-40; The Quality
menting and communicating orders aimed at main- Standards Subcommittee of the American Academy of Neurology.
taining organ viability, coordinating organ allocation, Neurology 1995;45(5):1012-4.
contacting organ recovery teams from the designated
recipients’ facilities, and scheduling the operating
room for the recovery of organs. From this point on, and compares this information with a national data-
all orders are written by the coordinator; the attend- base of patients in need of organs that is maintained
ing and consulting physicians are no longer involved. by UNOS’s Organ Center. Patients awaiting an
The OPO coordinator will take a complete his- organ are compared with the donor in areas such as
tory of the donor (both from the information in the blood and tissue type, weight, age, and urgency of
patient’s chart and from staff nurses and physicians medical need, as well as the length of time the patient
and possibly family members). Previous laboratory has been on the waiting list. Proximity to the donor
results will be evaluated, and several additional is a major factor as well.
studies (such as liver and kidney function studies
and blood tests to assess pancreatic enzyme and thy- NURSING IMPLICATIONS OF BRAIN DEATH
roid hormone levels) are often ordered to guide The brain is in charge of the proper functioning of
treatment. A central line or pulmonary artery all body systems. In a patient who is brain dead,
therefore, keeping the donor organs viable involves,
in a sense, fooling the body into thinking the brain
is still functioning. The nurse’s goals in this regard
When a patient is a potential or are determined by the following changes as they
take place in various organ systems. (It should be
designated organ donor, the nursing noted that because there is scant research in the lit-
erature pertaining to humans, most of the research
care required may be even more cited in this article was conducted in animals.)
The brain. Normal responses to any sympathetic
rigorous after brain death than stimulation include increases in blood pressure,
heart rate, cardiac contractility, minute ventilation
before such death occurs. (the volume of air per minute that moves in and out
of the lungs), and peripheral vasomotor tone.
Catecholamines also “promote platelet aggregation,
accompanied by serotonin release.”26 Serotonin has
catheter may be inserted for hemodynamic monitor- vasospastic effects on coronary arteries. Both
ing.5 The additional testing is labor intensive; often platelet aggregation and vasospasticity reduce coro-
the donor’s condition deteriorates so rapidly that nary artery blood flow.
additional nurses are needed to perform stabilizing Almost immediately after brain death, activation
tasks such as the monitoring of fluids and vital signs of the sympathoadrenal axis causes a great increase
and the administration of drugs and fluids. in the levels of circulating catecholamines.15, 17, 18
The staff nurse reports all aberrancies in the During this sympathetic storm, circulating dopa-
donor’s condition to the OPO coordinator, who, in mine levels have been shown to increase by as much
turn, provides orders for their correction. If the coor- as 800%, epinephrine levels by as much as 700%,
dinator isn’t available, the nurse may make treatment and norepinephrine levels by up to 100%.17, 18 The
decisions based on a critical pathway designated by effects can be catastrophic to human tissue.
the coordinator. (One such pathway is UNOS’s Hypercapnia resulting from the cerebral hypoperfu-
Critical Pathway for the Organ Donor [www. sion that follows brain death also stimulates cate-
unos.org/resources/pdfs/CriticalPathwayPoster.pdf].) cholamine release.15
The coordinator reviews the laboratory test results Declining ADH. Infarction of the tissue of the
for the donor’s blood type and other serum markers hypothalamus eventually results in a decline in cir-
62 AJN ▼ March 2007 ▼ Vol. 107, No. 3 http://www.nursingcenter.com
culating antidiuretic hormone (ADH; also called
arginine vasopressin); this in turn affects the kid-
neys’ ability to concentrate urine and leads to dia- Organ-Procurement
betes insipidus.18, 20 The result is severe diuresis with
accompanying hypernatremia, hyperosmolarity, Organizations
and dehydration in up to 80% of cases of brain
death.16
Declining T3 and T4. Ordinarily, the hypothala-
T he National Organ Transplantation Act of 1984 cre-
ated a multidisciplinary task force to study organ
donation, procurement, and transplantation. It also
mus stimulates the pituitary to secrete thyroid- established a national organ sharing system, the Organ
stimulating hormone (TSH), which prompts the Procurement and Transplantation Network (OPTN),
thyroid to release triiodothyronine (T3) and its part- which has been administered since its inception by the
ner hormone, thyroxine (T4). After brain death, T3 United Network for Organ Sharing (www.unos.org), a
levels drop as a result of infarction in the tissues of national nonprofit organization. The Omnibus
the hypothalamus and pituitary.17 T4 levels appear Reconciliation Act of 1986 implemented many of the
to decline as well; Chen and colleagues found in a task force’s recommendations, including that organ-
study in dogs that levels of both T3 and T4 declined procurement organizations (OPOs) be members of the
significantly after brain death (although remaining OPTN. And in 1998, the Department of Health and
within normal limits) and suggested that such Human Services’ Health Care Financing Administration
decreases “could have contributed to post–brain issued Hospital Conditions of Participation for Organ
death cardiac dysfunction.”18 Other effects are not as Donation, which delineated criteria for reimbursement
well established. The decrease in T3 has been associ- under Medicare and Medicaid. To be in compliance,
ated with inhibited mitochondrial function, resulting hospitals must “have an agreement with an OPO,”
in poor cardiac contractility, anaerobic metabolism, “notify OPOs in a timely manner about patients who
and lactic acidosis following brain death.16 However, have died or whose death is imminent,” and collaborate
Chen and colleagues stated that although anaerobic with the OPO “to ensure every family is offered the
metabolism and metabolic acidosis were observed option of donation.”9
immediately after brain death in their canine study, Most OPOs are independent, although a few are hospi-
these were not associated with declining thyroid hor- tal based. An OPO team doesn’t recover organs itself; that
mone levels.18 is handled by organ recovery teams from the designated
Loss of thermoregulation. The hypothalamus recipients’ facilities. An OPO team’s responsibilities typi-
regulates body temperature through a homeostatic cally include9:
feedback mechanism. In a healthy person, if the • providing public and professional education on the
body becomes too hot, the hypothalamus prompts donation process.
vasodilation, resulting in sweating. If the body • evaluating the “medical suitability” of potential
becomes too cool, the hypothalamus prompts vaso- donors.
constriction in the skin, shivering, and piloerection, • with hospital staff, offering families the option of
resulting in heat retention. donation.
Systemic hypothermia—heat loss secondary to • managing and coordinating organ procurement and
massive peripheral vasodilation and loss of ther- allocation.
moregulatory control by the hypothalamus—is • providing support to donor families.
often seen after brain death.16 Without intervention, • maintaining documentation.
the donor’s body eventually assumes ambient tem-
perature; therefore, thermoregulation is a priority.20
Nursing implications. Treatment of diabetes
insipidus involves fluid replacement to offset hourly Medrol) 15 mg/kg IV bolus, which may be repeated
urine output and often includes an IV vasopressin in 24 hours if needed; and an insulin drip of 1 unit
(Pitressin) infusion as well. The nurse should be dili- per hour adjusted to maintain blood glucose at
gent in observing urine output (at a minimum, 0.5 between 120 and 180 mg/dL.25 Blood glucose
mL/kg/h) to determine whether the patient needs should be measured hourly to determine the need
fluid resuscitation, a vasopressin infusion, or both. for coverage with regular insulin or the initiation of
According to UNOS’s Critical Pathway for the an insulin drip.
Organ Donor, the following are essential to hor- Following the loss of thermoregulation, an IV
monal management in potential donors: T3 fluid warmer, a forced-air room warming device,
4 microgram IV bolus followed by an infusion of and warming blankets should be used to maintain
3 micrograms per hour; vasopressin 1 unit IV bolus the donor’s body temperature at 36.5°C to 37.5°C
followed by an infusion of 0.5 to 4 units per hour, (97.7°F to 99.5°F).25
adjusted to 800 to 1200 dyne/sec/cm5 for systemic The heart. The normal heart is innervated by
vascular resistance; methylprednisolone (Solu- both the sympathetic and parasympathetic branches
ajn@wolterskluwer.com AJN ▼ March 2007 ▼ Vol. 107, No. 3 63
of the autonomic nervous system. Sympathetic stim- Another study found evidence to suggest that the
ulation of both the sinoatrial (SA) and the atrioven- myocardial damage that occurs during brain death
tricular (AV) nodes originates in the medulla “may be related to endogenous catecholamine
oblongata. The sympathetic fibers in the heart release (possibly resulting in increased calcium
release norepinephrine, increasing heart rate and uptake by the myocardial cells), inducing various
contractility. Parasympathetic stimulation of the SA forms of myocyte necrosis.”31 The calcium ion Ca++
and AV nodes also originates in the medulla through is responsible for the normal excitation and contrac-
cranial nerve X (the vagus nerve). The parasympa- tion of myocardial tissue that results in the pumping
thetic fibers release acetylcholine, decreasing heart action of the myocardium. After brain death, the
rate and contractility. Cranial nerve IX (the glos- increased calcium uptake desensitizes the cardiac
sopharyngeal nerve) is also responsible for stimula- myofilaments to calcium, compromising cardiac con-
tion of cardiac events. These nerves are linked tractility and output.32
through connections to baroreceptors in the carotid The sympathetic storm also results in increased
arteries, controlling heart rate variability and arterial myocardial adenosine and lactate levels, which are
pressure. associated with myocardial dysfunction and
myocardial ischemia.16, 26, 33
Accumulation of neutrophils. In a canine study by
Chen and colleagues, they found that “irreversible
‘Uncoupling’ of the autonomic focal injuries and myocytolysis” occurred soon after
brain death.18 They also observed an “accumulation
and cardiovascular systems is and infiltration of neutrophils and subendocardial
hemorrhage,” as well as edema. Hemorrhage and
believed to be responsible for
edema may adversely affect the ability of the organ
the eventual cessation of cardiac to function fully after transplantation.
Altered gene expression. Yeh and colleagues
function after brain death. speculated that after brain death, “fluctuations in
catecholamine levels might act as important signals
in the subsequent alterations” in the expression of
myocardial genes that regulate functions such as
After brain death, the cardiovascular system is no contractility and growth.34 They hypothesized that
longer under autonomic control.27 The arterial the resulting malfunctions may be the cause of rejec-
baroreceptors that once allowed for automatic reg- tion or dysfunction of the donor heart after trans-
ulation of blood pressure and heart rate are no plantation. In a study with rabbits, they found that
longer functional.28 This “uncoupling” of the auto- “brain death–associated increases in expression of
nomic and cardiovascular systems is believed to be myocardial gene products” could be suppressed by
responsible for the eventual cessation of cardiac exogenous sympathetic blockade.34 Treatment with
function after brain death.27 During the first b-adrenergic blockers such as metoprolol (Lopressor)
Cushing response, “exaggerated uneven peripheral and labetalol (Normodyne, Trandate) is standard.
vasoconstriction” causes areas of hypoperfusion in Nursing implications. Exogenous catechol-
organ vasculature.15 However, the loss of autonomic amines, including epinephrine and dopamine, are
control soon causes “a decline in the sympathetic often used as inotropic agents to maintain blood
outflow to the blood vessels,”28 leading to vasodila- pressure and systemic perfusion. After brain death,
tion. A second hemodynamic collapse causes fur- epinephrine is usually infused at a standard dose
ther systemic vasodilation or vasoplegia, decreasing range of 0.05 to 1 micrograms per kilogram per
preload, adversely affecting afterload, and further minute; dopamine is infused at a standard dose
compromising cardiac output.17, 29 range of 5 to 10 micrograms per kilogram per
Increased catecholamines. Even in an adequately minute. It’s imperative that the potential donor’s
perfused heart, high catecholamine levels will actual, not estimated, weight be used in determining
decrease the myocardial cells’ ability to pump effec- the infusion dosage. Some OPO coordinators may
tively.30 Commenting on earlier studies, Herijgers want to estimate current weight by averaging the
and colleagues observed that “the severity of the patient’s weight on admission and her or his last
myocardial damage is correlated with the amount known weight. Patients often become severely edem-
of catecholamines released at the moment of brain atous during an ICU stay, with consequent and
death.”26 Catecholamines also are associated with sometimes marked increases in body weight. This
platelet aggregation and the release of serotonin; edema may dramatically change the effect of vaso-
this study suggests that brain death may cause pressors from therapeutic to toxic.
myocardial damage through vasospasm caused by The OPO coordinator should be notified of heart
the effects of serotonin release.26 rate, blood pressure, or central venous pressure lev-
64 AJN ▼ March 2007 ▼ Vol. 107, No. 3 http://www.nursingcenter.com
els that vary from limits established in the critical
pathway being used. Diagnostic evaluation of the Brain Death: Confirmatory
potential donor’s heart may be necessary to deter-
mine its viability for transplantation. Tests such as
Findings on Neurologic Assessment
echocardiography, transesophageal echocardiogra- Glasgow Coma Scale score: 3 (no eye, verbal, or
phy, or cardiac catheterization may be necessary motor responses to auditory or painful stimuli)
in older donors or those with concurrent illnesses in Apnea: a partial pressure of carbon dioxide > 60
order to visualize valves, heart wall motion, and mmHg off ventilator, no spontaneous breathing
overall function. (Although older age or a history of
illness does not necessarily preclude donation, each Absent pupillary reflex: pupils remain fixed and
case is evaluated on its own merits and at the coor- dilated, size > 4 mm, upon exposure to light
dinator’s discretion.) Absent oculovestibular reflex: eyes remain midline
The lungs. Breathing is controlled by the respira- when ear canal is irrigated with ice water 10 mL
tory center of the brain, an area located in the Absent oculocephalic (“doll’s eyes”) reflex: eyes
medulla oblongata and pons. In cases of traumatic remain fixed in position when head is turned from
brain injury, cerebral inflammation and edema side to side
cause infarction of the tissues of the respiratory cen- Absent corneal reflex: no blinking upon corneal stimu-
ter.15, 16, 35 Central apnea results.6 lation with cotton-tipped applicator
The sympathetic storm following brain death has
direct, detrimental effects on lung tissue. Increasing Absent gag reflex: no gag reflex upon manual manip-
systemic hypertension and left atrial pressure result ulation of patient’s trachea or upon deep endotra-
in elevated pulmonary capillary pressures and sub- cheal suctioning
sequent endothelial damage to these capillaries.16 Absent cough reflex: no cough reflex upon deep
Their permeability increases and fluid leaks into the endotracheal suctioning
alveoli and interstitium of the lungs. Fluid resuscita- Wijdicks EF. N Engl J Med 2001;344(16):1215-21; Sullivan J, et al.
tion of a patient who is hemodynamically compro- Crit Care Nurse 1999;19(2):37-9, 41-6.
mised further exacerbates pulmonary edema.16
Potential donors in whom oxygen saturation of
95% or greater on 100% oxygen cannot be
achieved or maintained, or those in whom lung tis- depleted, the body begins breaking down fat, lead-
sue viability is questionable, may undergo bron- ing to lactic acidosis.
choscopy so that lung tissue can be visualized to Nursing interventions include frequent assess-
determine its viability for transplantation. ment for diabetes insipidus, with treatment accord-
According to UNOS’s critical pathway, a state of ing to status, and fluid replacement according to the
mild respiratory alkalosis (partial pressure of car- parameters established by the OPO coordinator.
bon dioxide between 30 and 35 mmHg) is prefer- The pancreas. Insulin is normally secreted by the
able for potential donors.25 beta cells of the pancreas in response to blood glucose
Nursing implications. Peak airway pressures levels. Cranial nerve X also stimulates the production
should be maintained at less than 30 cm H2O.25 of pancreatic secretions. A study by Obermaier and
Accordingly, although ventilatory settings will be colleagues determined that brain death “causes sig-
controlled by the OPO coordinator and the respira- nificant pathophysiological alterations in the pan-
tory therapist, the nurse will monitor tidal volumes creas,” including deterioration of pancreatic
delivered to the patient, the inspiratory flow rate, microvasculature, inflammation, and histologic dam-
and the fraction of inspired oxygen. age.39 Each of these sequelae plays a role in disrupting
The liver. Blood flow to the liver has been found beta cell functioning, ultimately destroying the pan-
to decrease after brain death, but the implications of creas’s ability to secrete sufficient insulin.
this are unclear. One study found that “morpho- That a hyperglycemic state results after brain
logic change in the liver was slight” and that “the death is undisputed.16, 18, 40 Endocrine pancreatic
liver remained viable for as long as six hours follow- functions are normal after brain death, according to
ing brain death,”36 while another study found that Masson and colleagues, and hyperglycemia results
liver functions were impaired.37 The hyperosmolar- from tissue-insulin resistance,41 although further
ity associated with diabetes insipidus has been cor- study is needed to determine what causes the resis-
related with hepatocyte destruction and altered tance. Hyperglycemia may be complicated by the
hepatocyte mitochondria.38 large volume of glucose-containing fluids often used
The shift to anaerobic metabolism leads to a for fluid resuscitation to correct hypernatremia.16
depletion of liver glycogen.20 Organs must delve into Although the mechanism underlying the disruption
their own glycogen stores for the energy necessary of serum glucose regulation remains unclear, it is
to carry out normal cell functions; once these are well established that fluctuations occur.
ajn@wolterskluwer.com AJN ▼ March 2007 ▼ Vol. 107, No. 3 65
Nursing implications. Hyperglycemia can lead to 5. Wheeldon DR, et al. Transforming the “unacceptable”
osmotic diuresis and cellular dehydration, resulting donor: outcomes from the adoption of a standardized donor
management technique. J Heart Lung Transplant 1995;
in hypovolemia. Regular blood-glucose monitoring 14(4):734-42.
with corrective interventions is crucial. Finger-stick 6. A definition of irreversible coma. Report of the Ad Hoc
measurement is usually adequate. Insulin should Committee of the Harvard Medical School to Examine the
Definition of Brain Death. JAMA 1968;205(6):337-40.
be administered at a minimum rate of 1 unit per
7. Guidelines for the determination of death. Report of the
hour, adjusted to keep blood glucose between 120 medical consultants on the diagnosis of death to the
and 180 mg/dL.25 President’s Commission for the Study of Ethical Problems in
Medicine and Biomedical and Behavioral Research. JAMA
The kidneys. One study with rats found that, 1981;246(19):2184-6.
immediately after brain death, severe vasoconstric- 8. Capron AM. Brain death—well settled yet still unresolved.
tion occurred, causing increased regional vascular N Engl J Med 2001;344(16):1244-6.
resistance.42 Renal vascular resistance was especially 9. Chabalewski F, et al. Policy and practice in organ transplan-
high, rising to four times higher than normal. Such tation. In: Organ transplantation: concepts, issues, practice,
and outcomes. Medscape; 2002. http://www.medscape.com/
markedly heightened vascular resistance can cause viewpublication/704_about.
ischemia. Perfusion to abdominal organs also 10. Practice parameters for determining brain death in adults
decreases as a result of vasoconstriction.19 (summary statement). The Quality Standards Subcommittee
of the American Academy of Neurology. Neurology 1995;
Under normal conditions, hypoperfusion of the 45(5):1012-4.
kidneys activates the renin–angiotensin–aldosterone 11. Lock M. Inventing a new death and making it believable.
system, resulting in vasoconstriction and salt and Anthropology and Medicine 2002;9(2):97-115.
water retention. The activation of the renin– 12. Wijdicks EF. Determining brain death in adults. Neurology
1995;45(5):1003-11.
angiotensin–aldosterone system after brain death
13. Wijdicks EF. The diagnosis of brain death. N Engl J Med
further exacerbates vasoconstriction and compro- 2001;344(16):1215-21.
mises renal blood flow. Eventually renal insuffi- 14. Dominguez-Roldan JM, et al. Changes in the intracranial
ciency results, possibly compromising kidney pulse pressure waveform associated with brain death.
Transplant Proc 1999;31(6):2597-8.
viability and posttransplantation function.
15. Shoemaker WC, et al. Hemodynamic and oxygen metabolic
Cardiovascular collapse following the sympa- patterns in brain death after head trauma. Russian
thetic storm and lack of ADH leading to diabetes Neurosurgery 2002;3(8). http://www.neuro.neva.ru/English/
Issues/Articles_3_2002/zelman.htm.
insipidus may also cause significant renal hypoper-
16. Smith M. Physiologic changes during brain stem death—
fusion. Significant, irreversible glomerular and lessons for management of the organ donor. J Heart Lung
tubular injury will follow if renal perfusion is not Transplant 2004;23(9 Suppl):S217-22.
restored. 17. Chiari P, et al. Biphasic response after brain death induction:
prominent part of catecholamines release in this phenome-
Nursing interventions that maintain hemody- non. J Heart Lung Transplant 2000;19(7):675-82.
namic stability and replace volume best ensure 18. Chen EP, et al. Hormonal and hemodynamic changes in a
renal-tissue viability for transplantation. IV infu- validated animal model of brain death. Crit Care Med
sions of diuretics for oliguria or antidiuretics for 1996;24(8):1352-9.
diabetes insipidus, at levels set by the OPO coordi- 19. Smith SL. Organ and tissue donation and recovery. In:
Organ transplantation: concepts, issues, practice, and
nator in accordance with the critical pathway being outcomes. Medscape; 2003. http://www.medscape.com/
used, may be warranted. Fluid intake and urine out- viewpublication/704_about.
put should be closely monitored, as well as the 20. Marshall VC. Pathophysiology of brain death: effects on
allograft function. Transplant Proc 2001;33(1-2):845-6.
patient’s overall state of hydration. Hydration can 21. Bittner HB, et al. A valid experimental brain death organ
be monitored noninvasively by frequent measure- donor model. J Heart Lung Transplant 1995;14(2):308-17.
ment of urine output, heart rate, and blood pres- 22. Sullivan J, et al. Determining brain death. Crit Care Nurse
sure, and invasively by using a central line to 1999;19(2):37-9, 41-6.
monitor central venous pressure. ▼ 23. Huang AH. The hot nose sign. Radiology 2005;235(1):216-7.
24. Conrad GR, Sinha P. Scintigraphy as a confirmatory test of
brain death. Semin Nucl Med 2003;33(4):312-23.
REFERENCES
25. United Network for Organ Sharing. Critical pathway for the
1. United Network for Organ Sharing. Data. The Network. organ donor. The Network. 2002. http://www.
2006. http://www.unos.org/data. unos.org/resources/pdfs/CriticalPathwayPoster.pdf.
2. Organ Donation Breakthrough Collaborative. About the col- 26. Herijgers P, et al. Endothelial activation through brain
laborative: charter for the Organ Donation Breakthrough death? J Heart Lung Transplant 2004;23(9 Suppl):S234-9.
Collaborative. U.S. Department of Health and Human
Services. 2003. http://www.organdonationnow.org/index. 27. Goldstein B, et al. Uncoupling of the autonomic and cardio-
cfm?fuseaction=Page.viewPage&pageId=471. vascular systems in acute brain injury. Am J Physiol
1998;275(4 Pt 2):R1287-92.
3. National Women’s Health Information Center. Frequently
asked questions about women’s health: organ donation and 28. Kuo TB, et al. Diminished vasomotor component of sys-
transplantation. Office on Women’s Health, U.S. Department temic arterial pressure signals and baroreflex in brain death.
of Health and Human Services. 2006. http://www.4woman. Am J Physiol 1997;273(3 Pt 2):H1291-8.
gov/faq/organ_donation.htm. 29. Szabo G. Physiologic changes after brain death. J Heart
4. Lopez-Navidad A, et al. Organ shortage: viability of poten- Lung Transplant 2004;23(9 Suppl):S223-6.
tial organ donors and possible loss depend on health care 30. Smith JM, Pilati CF. Effect of massive sympathetic nervous
workers who are responsible for the organ procurement pro- system activation on coronary blood flow and myocardial
gram. Transplant Proc 1997;29(8):3614-6. energy pool. Exp Biol Med (Maywood) 2002;227(2):125-32.
66 AJN ▼ March 2007 ▼ Vol. 107, No. 3 http://www.nursingcenter.com
31. Novitzky D, et al. Prevention of myocardial injury during
brain death by total cardiac sympathectomy in the Chacma
baboon. Ann Thorac Surg 1986;41(5):520-4.
32. Szabo G, et al. Role of neural and humoral factors in hyper-
dynamic reaction and cardiac dysfunction following brain
3.5 HOURS
Continuing Education
death. J Heart Lung Transplant 2000;19(7):683-93.
33. Ryan JB, et al. Functional evidence of reversible ischemic
EARN CE CREDIT ONLINE
Go to www.nursingcenter.com/CE/ajn and receive a certificate within minutes.
injury immediately after the sympathetic storm associated
with experimental brain death. J Heart Lung Transplant
2003;22(8):922-8.
34. Yeh T, Jr., et al. Central sympathetic blockade ameliorates
brain death-induced cardiotoxicity and associated changes in GENERAL PURPOSE: To explain for registered professional
myocardial gene expression. J Thorac Cardiovasc Surg nurses how brain death is determined in adults and how
2002;124(6):1087-98. potential organ donors are identified, and to describe
35. Takada M, et al. Effects of explosive brain death on cytokine essential nursing interventions.
activation of peripheral organs in the rat. Transplantation
1998;65(12):1533-42. LEARNING OBJECTIVES: After reading this article and taking
36. Imai K, et al. Experimental evaluation of hepatic circulation, the test on the next page, you will be able to
energy metabolism, and morphologic changes in brain death. • describe the process of managing potential organ
Transplant Proc 1998;30(7):3282-3. donors who have been declared brain dead.
37. Onumata O, et al. Effects of hypotension on hepatic circula- • outline the pathophysiologic changes that occur follow-
tion and function: comparison of brain death and exsan- ing brain death.
guination models. Transplant Proc 2000;32(7):2293-6. • review the criteria and diagnostic parameters that define
38. Florman SS, et al. Hyperosmolarity associated with diabetes brain death.
insipidus alters hepatocyte structure and function but not
survival after orthotopic liver transplantation in rats. TEST INSTRUCTIONS
Transplantation 1998;65(1):36-41. To take the test online, go to our secure Web site at www.
39. Obermaier R, et al. Brain death impairs pancreatic microcir- nursingcenter.com/CE/ajn.
culation. Am J Transplant 2004;4(2):210-5. To use the form provided in this issue,
40. Masson F, et al. Thyroid function in brain-dead donors. • record your answers in the test answer section of the CE
Transpl Int 1990;3(4):226-33. enrollment form between pages 64 and 65. Each ques-
41. Masson F, et al. The endocrine pancreas in brain-dead tion has only one correct answer. You may make copies
donors. A prospective study in 25 patients. Transplantation of the form.
1993;56(2):363-7. • complete the registration information and course evalua-
42. Herijgers P, et al. Changes in organ perfusion after brain tion. Mail the completed enrollment form and registration
death in the rat and its relation to circulating catechol- fee of $27.95 to Lippincott Williams and Wilkins CE
amines. Transplantation 1996;62(3):330-5. Group, 2710 Yorktowne Blvd., Brick, NJ 08723, by
March 31, 2009. You will receive your certificate in four to
six weeks. For faster service, include a fax number and we
will fax your certificate within two business days of receiv-
ing your enrollment form. You will receive your CE certifi-
cate of earned contact hours and an answer key to review
your results. There is no minimum passing grade.
DISCOUNTS and CUSTOMER SERVICE
• Send two or more tests in any nursing journal published by
Lippincott Williams and Wilkins (LWW) together, and
deduct $0.95 from the price of each test.
• We also offer CE accounts for hospitals and other health
care facilities online at www.nursingcenter.com. Call
(800) 787-8985 for details.
PROVIDER ACCREDITATION
LWW, publisher of AJN, will award 3.5 contact hours
for this continuing nursing education activity.
LWW is accredited as a provider of continuing nursing
education by the American Nurses Credentialing Center’s
Commission on Accreditation.
LWW is also an approved provider of continuing nurs-
ing education by the American Association of Critical-
Care Nurses #00012278 (CERP category A), District of
Columbia, Florida #FBN2454, and Iowa #75. LWW
home study activities are classified for Texas nursing con-
tinuing education requirements as Type 1. This activity
is also provider approved by the California Board of
Registered Nursing, provider number CEP 11749, for
3.5 contact hours.
Your certificate is valid in all states.
TEST CODE: AJN0607
ajn@wolterskluwer.com AJN ▼ March 2007 ▼ Vol. 107, No. 3 67
Вам также может понравиться
- Perioperative Management of The Organ Donor After Diagnosis of Death Using Neurological CriteriaДокумент7 страницPerioperative Management of The Organ Donor After Diagnosis of Death Using Neurological Criterialoshaana105Оценок пока нет
- The Dead Donor Rule and Organ Transplantation: PerspectiveДокумент2 страницыThe Dead Donor Rule and Organ Transplantation: Perspectivediego cruzadoОценок пока нет
- Addressing Limitations of Time and Resources in The EmergencyДокумент10 страницAddressing Limitations of Time and Resources in The EmergencyblitzcanoОценок пока нет
- Anestesia en Procuracion de OrganosДокумент11 страницAnestesia en Procuracion de OrganosIvan MoralesОценок пока нет
- Nejm.231204.care Organ DonorДокумент10 страницNejm.231204.care Organ DonorMarisol Gallego DuqueОценок пока нет
- Neurocriticalcareresearch: Collaborations For Curing ComaДокумент8 страницNeurocriticalcareresearch: Collaborations For Curing ComaJonathan Mendoza V.Оценок пока нет
- Consensus Statement On Brain Death - Malaysia - 2003Документ25 страницConsensus Statement On Brain Death - Malaysia - 2003docpunit100% (1)
- LampiranДокумент9 страницLampiranNYONGKERОценок пока нет
- ProspektifДокумент3 страницыProspektifElsa Indah SuryaniОценок пока нет
- Molecular Genetics of Human MicrocephalyДокумент7 страницMolecular Genetics of Human MicrocephalymohsinОценок пока нет
- NSG 700 - Organ TranspantДокумент30 страницNSG 700 - Organ TranspantJellou MacОценок пока нет
- Bioethical Issues Concerning DeathДокумент8 страницBioethical Issues Concerning DeathShirin Kay ButaОценок пока нет
- Literature Review Head InjuryДокумент5 страницLiterature Review Head Injuryafmzinuvouzeny100% (1)
- Forum: Therapeutic Hope, Spiritual Distress, and The Problem of Stem Cell TourismДокумент4 страницыForum: Therapeutic Hope, Spiritual Distress, and The Problem of Stem Cell TourismRio Fajar ImanОценок пока нет
- Organ Transplantation Legal, Ethical and Islamic Perspective in NigeriaДокумент13 страницOrgan Transplantation Legal, Ethical and Islamic Perspective in NigeriaMuaz ShukorОценок пока нет
- Brain DeathДокумент4 страницыBrain DeathArdhi Oemar AgustjikОценок пока нет
- 9096 31639 1 PBДокумент5 страниц9096 31639 1 PBjhuОценок пока нет
- Traumatic Brain Injury in Adults and ChildrenДокумент36 страницTraumatic Brain Injury in Adults and ChildrenShakib ShafiОценок пока нет
- Bioethics Lecture01Документ43 страницыBioethics Lecture01Jm CasupangОценок пока нет
- Jurnal Kita ForensikДокумент5 страницJurnal Kita ForensikYudhi Aulia ZulfatanОценок пока нет
- Stiell Et Al 2014 What Is The Optimal Chest Compression Depth During Out of Hospital Cardiac Arrest Resuscitation ofДокумент9 страницStiell Et Al 2014 What Is The Optimal Chest Compression Depth During Out of Hospital Cardiac Arrest Resuscitation oftempeuedanОценок пока нет
- Chapter 9 NotesДокумент10 страницChapter 9 NotesNapao Camelle Ann C.Оценок пока нет
- Coma Causas ReversíveisДокумент13 страницComa Causas ReversíveisRuan BicalhoОценок пока нет
- Perspective: New England Journal MedicineДокумент3 страницыPerspective: New England Journal MedicineAmy WooОценок пока нет
- Frailty For Neurologists - A Practical GuideДокумент8 страницFrailty For Neurologists - A Practical GuideAlphaОценок пока нет
- Despertar AnestésicoДокумент7 страницDespertar AnestésicoMontserratdelaRosaОценок пока нет
- Organ TransplantationДокумент6 страницOrgan TransplantationFares SamirОценок пока нет
- 9.1 Organ Donation and Brain DeathДокумент8 страниц9.1 Organ Donation and Brain DeathΜατθαίος ΠαππάςОценок пока нет
- IPCR Research: Any Offers?: Endocrine Et Al J PsychopharmacologyДокумент2 страницыIPCR Research: Any Offers?: Endocrine Et Al J PsychopharmacologyMj ManuelОценок пока нет
- Ứng dụng thuyết nhu cầu maslow trong chăm sóc bệnh nhânДокумент7 страницỨng dụng thuyết nhu cầu maslow trong chăm sóc bệnh nhânDieu LinhОценок пока нет
- Challenges in Organ TransplantationДокумент10 страницChallenges in Organ TransplantationBrie100% (1)
- 10.1001@jama.2020.3593 Brain DeathДокумент2 страницы10.1001@jama.2020.3593 Brain DeathSardono WidinugrohoОценок пока нет
- Jamaneurology Burke 2019 VP 190011Документ2 страницыJamaneurology Burke 2019 VP 190011joao victorОценок пока нет
- Magnus Et Al. - Accepting Brain DeathДокумент4 страницыMagnus Et Al. - Accepting Brain DeathDoopОценок пока нет
- Chapter 3Документ151 страницаChapter 3ManojОценок пока нет
- Transplantation and RegenerativeДокумент3 страницыTransplantation and RegenerativeMustakim SPОценок пока нет
- Hennemann (2021)Документ6 страницHennemann (2021)Nerea AlvarezОценок пока нет
- Listen To Patient and CollagueДокумент2 страницыListen To Patient and CollagueVITRIA NOVITA SARIОценок пока нет
- Debate (Speech)Документ5 страницDebate (Speech)Jessie GlennОценок пока нет
- Certification of Brain Stem Death in India - Medico-Legal PerspectiveДокумент6 страницCertification of Brain Stem Death in India - Medico-Legal PerspectiveRTОценок пока нет
- Jurnal 3Документ7 страницJurnal 3kampret berbagiОценок пока нет
- Developing A Therapeutic Approach Toward Active Engagement For Veterans With Mild Traumatic Brain Injury (Tapia Et Al., 2019)Документ9 страницDeveloping A Therapeutic Approach Toward Active Engagement For Veterans With Mild Traumatic Brain Injury (Tapia Et Al., 2019)T4H ResearchОценок пока нет
- Chinese Harvesting Organs From Prisoners Who Are AliveДокумент9 страницChinese Harvesting Organs From Prisoners Who Are AliveMichael SmithОценок пока нет
- Literature Review of Post-Traumatic Stress Disorder in The Critical Care PDFДокумент14 страницLiterature Review of Post-Traumatic Stress Disorder in The Critical Care PDFOriza Zara SativaОценок пока нет
- Transplantation: J. Med. EthicsДокумент3 страницыTransplantation: J. Med. EthicsFuraya FuisaОценок пока нет
- Brain Metastases: Review ArticleДокумент17 страницBrain Metastases: Review ArticleSebastianОценок пока нет
- Clinical Review: Care of The Dying Patient: The Last Hours or Days of LifeДокумент5 страницClinical Review: Care of The Dying Patient: The Last Hours or Days of LifevabcunhaОценок пока нет
- Anesthetic Considerations of Organ Procurement After Brain and Cardiac Death A Narrative ReviewДокумент14 страницAnesthetic Considerations of Organ Procurement After Brain and Cardiac Death A Narrative Reviewnvidia coreОценок пока нет
- Emily Risner - Research Essay PDFДокумент10 страницEmily Risner - Research Essay PDFapi-455396636Оценок пока нет
- Running Head: Animal Organs As Transplants in Humans 1Документ4 страницыRunning Head: Animal Organs As Transplants in Humans 1Lydiah KimaniОценок пока нет
- DS7. 1-s2.0-S193459091300146X-mainДокумент3 страницыDS7. 1-s2.0-S193459091300146X-mainImro'atul MuttafiahОценок пока нет
- Dnar LANGUAGE Is ImportantДокумент5 страницDnar LANGUAGE Is Importantjorgeroca2009Оценок пока нет
- 10 Encephalopathy - Approach To Evaluation - 2005Документ16 страниц10 Encephalopathy - Approach To Evaluation - 2005Evelyn Lee RussellОценок пока нет
- The Importance of Diagnosing and Managing ICU DeliriumДокумент13 страницThe Importance of Diagnosing and Managing ICU DeliriumPablo RamirezОценок пока нет
- Article 1Документ28 страницArticle 1Prateek Kumar PandaОценок пока нет
- Case StudyДокумент73 страницыCase StudyClark LlameraОценок пока нет
- A Ann CraniotomyДокумент41 страницаA Ann CraniotomyF̳̿a̳̿l̳̿a̳̿h̳̿ Opcional S̳̿u̳̿d̳̿i̳̿r̳̿a̳̿d̳̿i̳̿r̳̿e̳̿j̳̿a̳̿Оценок пока нет
- Organ DonationДокумент34 страницыOrgan Donationapi-404314061Оценок пока нет
- Behavioral Health NeurpsycatricДокумент297 страницBehavioral Health NeurpsycatricRohit SagarОценок пока нет
- eSP EchoДокумент18 страницeSP EchoBeck100% (1)
- Computational Models For The Human Body PDFДокумент679 страницComputational Models For The Human Body PDFGuilherme AyresОценок пока нет
- Healing The Angry BrainДокумент1 страницаHealing The Angry BrainMari AssisОценок пока нет
- Oral CavityДокумент65 страницOral Cavityugwuokeprince4Оценок пока нет
- Nursing Care of A Family Experiencing A Sudden Pregnancy ComplicationДокумент5 страницNursing Care of A Family Experiencing A Sudden Pregnancy ComplicationCrisheila Sarah PiedadОценок пока нет
- Nutrition QuizДокумент3 страницыNutrition QuizAnonymous h2EnKyDb100% (1)
- Excel Sheet For First Aid 2014 For USMLE Step 1 PagesДокумент2 страницыExcel Sheet For First Aid 2014 For USMLE Step 1 Pageswecan12345Оценок пока нет
- Carbon Dioxide MSDSДокумент12 страницCarbon Dioxide MSDSRaja DhanasekaranОценок пока нет
- Gen EdДокумент57 страницGen EdCeasar Ryan AsuncionОценок пока нет
- Yerba Mate - An Overview of Physiological Effects in HumansДокумент13 страницYerba Mate - An Overview of Physiological Effects in HumansJuanManuelCabarcosОценок пока нет
- Cns Neurological ExaminationДокумент26 страницCns Neurological ExaminationDr.P.NatarajanОценок пока нет
- MR Pulse SequencesДокумент125 страницMR Pulse SequencesdrphducОценок пока нет
- Physiology of DigestionДокумент23 страницыPhysiology of DigestionLàXsun ShrèsthàОценок пока нет
- Fish Diseases FactsheetДокумент2 страницыFish Diseases FactsheetWayneОценок пока нет
- Protein Energy Malnutrition (PEM)Документ39 страницProtein Energy Malnutrition (PEM)CLEMENT100% (3)
- Biology 2A03: Introduction To Physiology & HomeostasisДокумент409 страницBiology 2A03: Introduction To Physiology & Homeostasisampedm100% (8)
- Burns NeliganДокумент45 страницBurns NeliganroyvillafrancaОценок пока нет
- Reticulocyte CountДокумент25 страницReticulocyte CountMahmoud RamlawiОценок пока нет
- Komunikasi TerapeutikДокумент39 страницKomunikasi TerapeutikPratiwi AyuningtyasОценок пока нет
- Photosynthesis Class 10Документ14 страницPhotosynthesis Class 10shreya morajkarОценок пока нет
- Centric RelationДокумент7 страницCentric RelationHarish KumarОценок пока нет
- FAT Soluble VitaminsДокумент53 страницыFAT Soluble VitaminsFaria LatifОценок пока нет
- Biology Term 2 Practicals - ATPROДокумент12 страницBiology Term 2 Practicals - ATPROPratibha GuptaОценок пока нет
- Life Process Nutrition Question 1Документ3 страницыLife Process Nutrition Question 1Nakshatra PaliwalОценок пока нет
- Structure and Function of The Sympathetic Nervous SystemДокумент2 страницыStructure and Function of The Sympathetic Nervous SystemAnthony LopezОценок пока нет
- Acute Phase ProteinsДокумент380 страницAcute Phase ProteinsRogerio CansiОценок пока нет
- Lesson 1 "Modern Health Problems": A. Before-Reading ActivitiesДокумент3 страницыLesson 1 "Modern Health Problems": A. Before-Reading ActivitiesRomantische BohemienОценок пока нет
- IGCSE Answers Chapters 01 05Документ7 страницIGCSE Answers Chapters 01 05María Eugenia MolteniОценок пока нет
- Embryology HistoryДокумент18 страницEmbryology HistoryMelissa Monique Peart-Yates100% (1)
- Yoga BeginnerДокумент26 страницYoga BeginnerLuwani LinoОценок пока нет