Вам также может понравиться
- Gug Nani 2011Документ8 страницGug Nani 2011danielstevenОценок пока нет
- Detectionactivity Assessmentand Diagnosisofdental CarieslesionsДокумент15 страницDetectionactivity Assessmentand Diagnosisofdental CarieslesionsDrSugandh MittalОценок пока нет
- Jaja DallДокумент9 страницJaja DallDr.Anish RoyОценок пока нет
- Oral Oncology: Juan Seoane Lestón, Pedro Diz DiosДокумент5 страницOral Oncology: Juan Seoane Lestón, Pedro Diz DiosSULTAN1055Оценок пока нет
- 補充1 s2.0 S0300571215000494 mainДокумент10 страниц補充1 s2.0 S0300571215000494 mainVictor FanОценок пока нет
- Australian Dental Journal - 2009 - Evans - The Caries Management System An Evidence Based Preventive Strategy For DentalДокумент9 страницAustralian Dental Journal - 2009 - Evans - The Caries Management System An Evidence Based Preventive Strategy For DentalHarjotBrarОценок пока нет
- Metode de DiagnosticДокумент10 страницMetode de DiagnosticDorina IonescuОценок пока нет
- Vitali - 2021 - Asociación Entre Tto Ortodoncia y Cambios PulparesДокумент14 страницVitali - 2021 - Asociación Entre Tto Ortodoncia y Cambios PulparesMICHAEL ERNESTO QUINCHE RODRIGUEZОценок пока нет
- Detection and Diagnosis of The Early Caries Lesion: Proceedings Open AccessДокумент7 страницDetection and Diagnosis of The Early Caries Lesion: Proceedings Open AccessSamuelHpОценок пока нет
- Velscope Oral PremalignancyДокумент5 страницVelscope Oral PremalignancySusanaSanoОценок пока нет
- InTech-Traditional and Novel Caries Detection MethodsДокумент25 страницInTech-Traditional and Novel Caries Detection MethodsPaulette Sarmiento RosalesОценок пока нет
- Advances in Periodontal Surgery: A Clinical Guide to Techniques and Interdisciplinary ApproachesОт EverandAdvances in Periodontal Surgery: A Clinical Guide to Techniques and Interdisciplinary ApproachesSalvador NaresОценок пока нет
- Chairside Diagnosis of Periodontal Diseases A ReviewДокумент4 страницыChairside Diagnosis of Periodontal Diseases A ReviewEditor IJTSRDОценок пока нет
- Radiographic Diagnosis of Dental Caries: S. Brent Dove, D.D.S., M.SДокумент6 страницRadiographic Diagnosis of Dental Caries: S. Brent Dove, D.D.S., M.Saulia lubisОценок пока нет
- 1 s2.0 S030057121830099X MainДокумент8 страниц1 s2.0 S030057121830099X Mainkiara wardanaОценок пока нет
- Assessment of Oral Premalignancy Using Elastic Scattering SpectrosДокумент7 страницAssessment of Oral Premalignancy Using Elastic Scattering SpectrosYerly Ramirez MuñozОценок пока нет
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentОт EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraОценок пока нет
- Monitoring of Erosive Tooth WearДокумент5 страницMonitoring of Erosive Tooth Weartrain.with.asadhamoodОценок пока нет
- Strategies To Avoid Underdiagnosing Pit-And-Fissure Caries MitchellДокумент6 страницStrategies To Avoid Underdiagnosing Pit-And-Fissure Caries Mitchelljimmyboy111Оценок пока нет
- Tic Treatment of Teeth With Apical Period On Tit Is Single vs. Multi Visit TreatmentДокумент6 страницTic Treatment of Teeth With Apical Period On Tit Is Single vs. Multi Visit Treatmentgpv38Оценок пока нет
- Reliability of A New Caries Diagnostic System Differentiating Between Active and Inactive Caries LesionsДокумент10 страницReliability of A New Caries Diagnostic System Differentiating Between Active and Inactive Caries LesionsMariana Bastidas C.Оценок пока нет
- Interobserver and Intraobserver Variability in The Radiological Assessment of Sialolithiasis Using Cone Beam Computed TomographyДокумент5 страницInterobserver and Intraobserver Variability in The Radiological Assessment of Sialolithiasis Using Cone Beam Computed TomographydaruОценок пока нет
- Evans Article Caries in AdultДокумент10 страницEvans Article Caries in AdultInVision Dental-Models100% (2)
- E.C - Nithya - HistoryДокумент3 страницыE.C - Nithya - HistoryJeyachandran MariappanОценок пока нет
- Reliability, Validity, and Utility of Various Occlusal Measurement Methods and TechniquesДокумент7 страницReliability, Validity, and Utility of Various Occlusal Measurement Methods and TechniquesManjeev GuragainОценок пока нет
- PIIS0085253821005871Документ11 страницPIIS0085253821005871Renata CastroОценок пока нет
- Australian Dental Journal 2008 Caries Management SystemДокумент10 страницAustralian Dental Journal 2008 Caries Management Systemtea metaОценок пока нет
- Caries DiagnosisДокумент6 страницCaries DiagnosisAbhishek SoniОценок пока нет
- Sensitivity and Specificity of A Urine Circulating Anodic Antigen Test For The Diagnosis of Schistosoma Haematobium in Low Endemic SettingsДокумент19 страницSensitivity and Specificity of A Urine Circulating Anodic Antigen Test For The Diagnosis of Schistosoma Haematobium in Low Endemic SettingsPutraKakaОценок пока нет
- Error Reduction and Prevention in Surgical PathologyОт EverandError Reduction and Prevention in Surgical PathologyRaouf E. NakhlehОценок пока нет
- Molecular Methods Used in Clinical Laboratory: Prospects and PitfallsДокумент8 страницMolecular Methods Used in Clinical Laboratory: Prospects and PitfallsRon VitorОценок пока нет
- Introduction To BiomarkersДокумент83 страницыIntroduction To BiomarkersSubodh NanavatiОценок пока нет
- Endodontic Treatment of Teeth With Apical Periodontitis: Single vs. Multivisit TreatmentДокумент6 страницEndodontic Treatment of Teeth With Apical Periodontitis: Single vs. Multivisit TreatmentDaniel VivasОценок пока нет
- Eye Rubbing in The Aetiology of Keratoconus A Systematic Review PDFДокумент11 страницEye Rubbing in The Aetiology of Keratoconus A Systematic Review PDFMaria Jose SanjinesОценок пока нет
- Oup Accepted Manuscript 2016Документ11 страницOup Accepted Manuscript 2016Alvionita AnggrainyОценок пока нет
- SIJMedLife 07 18Документ6 страницSIJMedLife 07 18SmithaОценок пока нет
- Prashanth Panta - Oral Cancer Detection - Novel Strategies and Clinical Impact-Springer International Publishing (2019) PDFДокумент315 страницPrashanth Panta - Oral Cancer Detection - Novel Strategies and Clinical Impact-Springer International Publishing (2019) PDFShantanu DixitОценок пока нет
- Research Article: Sensing of Tooth Microleakage Based On Dental Optical Coherence TomographyДокумент7 страницResearch Article: Sensing of Tooth Microleakage Based On Dental Optical Coherence Tomography5054 - Monish SОценок пока нет
- Dental Caries An Update Medical Model Risk AssesmentДокумент6 страницDental Caries An Update Medical Model Risk AssesmentJuan Andres EspinozaОценок пока нет
- Diagnostic Evidence Cooperatives: Bridging The Valley of Death in Diagnostics DevelopmentДокумент3 страницыDiagnostic Evidence Cooperatives: Bridging The Valley of Death in Diagnostics DevelopmentNadia AyuningtiasОценок пока нет
- Validation of Quantitative Light-Induced Fluorescence-Digital (QLF-D) For The Detection of Approximal Caries in VitroДокумент8 страницValidation of Quantitative Light-Induced Fluorescence-Digital (QLF-D) For The Detection of Approximal Caries in VitroSelçuk ÖnalОценок пока нет
- Update On Gout 2012:, Nathalie BussoДокумент5 страницUpdate On Gout 2012:, Nathalie BussoMoha MohaОценок пока нет
- Icdas IДокумент9 страницIcdas IBharath RatnakaramОценок пока нет
- Jo2015 218280Документ6 страницJo2015 218280Akansh DattaОценок пока нет
- Nyvad 1999Документ9 страницNyvad 1999Felipe Maldonado ArayaОценок пока нет
- The Specific Identification of Staphylococcus Aureus With New Fluorescence in Situ Hybridization (FISH) MethodsДокумент163 страницыThe Specific Identification of Staphylococcus Aureus With New Fluorescence in Situ Hybridization (FISH) MethodstomxlawsonОценок пока нет
- Rapid On-site Evaluation (ROSE): A Practical GuideОт EverandRapid On-site Evaluation (ROSE): A Practical GuideGuoping CaiОценок пока нет
- NewCariesDiagnosticMethodsДокумент9 страницNewCariesDiagnosticMethodsKarma YogaОценок пока нет
- Minimal Intervention Dentistry: Part 4. Detection and Diagnosis of Initial Caries LesionsДокумент7 страницMinimal Intervention Dentistry: Part 4. Detection and Diagnosis of Initial Caries LesionsAdriana Paola Vega YanesОценок пока нет
- Radiographic caries detection accuracy meta-analysisДокумент10 страницRadiographic caries detection accuracy meta-analysisJae ConsiderОценок пока нет
- Assessing accuracy of ICDAS-II for detecting early occlusal cariesДокумент6 страницAssessing accuracy of ICDAS-II for detecting early occlusal cariesPatricio MendezОценок пока нет
- 21 Principles of Differential Diagnosis and Biopsy PETERSON HUPPДокумент22 страницы21 Principles of Differential Diagnosis and Biopsy PETERSON HUPPCecília MenezesОценок пока нет
- Advancement in Diagnostic Aids For Oral Premalignant Lesions: A ReviewДокумент5 страницAdvancement in Diagnostic Aids For Oral Premalignant Lesions: A ReviewAl RawdhaОценок пока нет
- A Protocol For Early Childhood Caries Diagnosis and Risk AssessmentДокумент9 страницA Protocol For Early Childhood Caries Diagnosis and Risk Assessmentmadhu kakanurОценок пока нет
- Role of Salivary BiomarkersДокумент48 страницRole of Salivary BiomarkersKevin FossОценок пока нет
- The Number of Karyorrhexis in PatientsДокумент5 страницThe Number of Karyorrhexis in PatientsAdhitya Sofiyati DewiОценок пока нет
- Mae 4262: Rockets and Mission Analysis: Combustion Overview For Rocket ApplicationsДокумент28 страницMae 4262: Rockets and Mission Analysis: Combustion Overview For Rocket ApplicationsmibarjanОценок пока нет
- Especificacion Tecnica Tanques FRP CANATUREДокумент3 страницыEspecificacion Tecnica Tanques FRP CANATURETomasae1980Оценок пока нет
- Manometer Pressure DifferenceДокумент5 страницManometer Pressure DifferenceBlue SkyОценок пока нет
- Grit Comparison ChartДокумент3 страницыGrit Comparison ChartAlex LomakovОценок пока нет
- Tissue Culture: Very Short Answer QuestionsДокумент4 страницыTissue Culture: Very Short Answer QuestionskzrdurОценок пока нет
- Refinery Wastewater Treatment TrainingДокумент27 страницRefinery Wastewater Treatment TrainingHariajahОценок пока нет
- Three Dimensional Numerical Simulation of Shell and Tube Heat Exchangers Part I Foundation and Fluid Mechanics PDFДокумент19 страницThree Dimensional Numerical Simulation of Shell and Tube Heat Exchangers Part I Foundation and Fluid Mechanics PDFAltamash MunirОценок пока нет
- MNL 67-2009 PDFДокумент128 страницMNL 67-2009 PDFlolo100% (2)
- FM-23-85 60mm Mortar M19 1967Документ174 страницыFM-23-85 60mm Mortar M19 1967rigal849Оценок пока нет
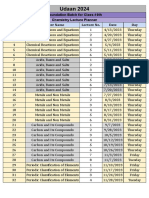
- Lecture Planner - Chemistry PDF OnlyДокумент1 страницаLecture Planner - Chemistry PDF OnlyJai ChandОценок пока нет
- Carbon Steel Flanges - Pressure and Temperature Ratings - Group 1.1 - Carbon SteelДокумент7 страницCarbon Steel Flanges - Pressure and Temperature Ratings - Group 1.1 - Carbon Steelnoha azamaliОценок пока нет
- Decolorization and Organic Removal From Palm Oil Mill Effluent by Fenton's ProcessДокумент5 страницDecolorization and Organic Removal From Palm Oil Mill Effluent by Fenton's Processagungtiyo21Оценок пока нет
- ReaPan 34G 38G ReagentДокумент2 страницыReaPan 34G 38G ReagentReaMetrixОценок пока нет
- API 2H Grade 50 Steel Plate SpecificationДокумент3 страницыAPI 2H Grade 50 Steel Plate SpecificationJym GensonОценок пока нет
- GLA0039 Final Report.926cd0f7Документ146 страницGLA0039 Final Report.926cd0f7Ntombi Langa-RoydsОценок пока нет
- Process Ventilation Design RequirementsДокумент4 страницыProcess Ventilation Design RequirementsMehman NasibovОценок пока нет
- Practice Quiz Diffraction 1Документ2 страницыPractice Quiz Diffraction 1pauljkt1Оценок пока нет
- Phase Inversion of W/O Emulsions by Adding Hydrophilic Surfactant - A Technique For Making Cosmetics ProductsДокумент8 страницPhase Inversion of W/O Emulsions by Adding Hydrophilic Surfactant - A Technique For Making Cosmetics ProductsAsshole FuckerОценок пока нет
- Reforming 2Документ15 страницReforming 2HAFIZ IMRAN AKHTERОценок пока нет
- GaN HEMTs - Advantages Opportunities and Challenges PDFДокумент60 страницGaN HEMTs - Advantages Opportunities and Challenges PDFghatakp2069Оценок пока нет
- Organic Chemistry Lab Prepares HydrocarbonsДокумент6 страницOrganic Chemistry Lab Prepares HydrocarbonsJhei Mesina AfableОценок пока нет
- HVAC Validation TestsДокумент4 страницыHVAC Validation TestsemonwreОценок пока нет
- Sibco CatalogueДокумент112 страницSibco CatalogueMonika SenОценок пока нет
- Amines PDFДокумент1 страницаAmines PDF최승원Оценок пока нет
- Niobium and Heat Affected Zone MythologyДокумент42 страницыNiobium and Heat Affected Zone MythologyLayzza TardinОценок пока нет
- Polyurea Resistance ChartДокумент1 страницаPolyurea Resistance ChartTanmay GorОценок пока нет
- Fatty Acids: Avid NnekenДокумент44 страницыFatty Acids: Avid NnekenCory AmeliaОценок пока нет
- ELITE™ AT 6900: The Dow Chemical Company - Enhanced Polyethylene ResinДокумент2 страницыELITE™ AT 6900: The Dow Chemical Company - Enhanced Polyethylene ResinLeductoan LeОценок пока нет
- Barett PDFДокумент20 страницBarett PDFlnadolskiОценок пока нет