Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- GMHP Claim Form - Online PDFДокумент4 страницыGMHP Claim Form - Online PDFSalem AmraneОценок пока нет
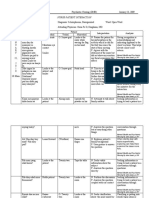
- Nurse-Patient Interaction: Mental Health and Psychiatric Nursing by Ann Isaacs p.197Документ4 страницыNurse-Patient Interaction: Mental Health and Psychiatric Nursing by Ann Isaacs p.197joey_gorgonioОценок пока нет
- Case Study MKTG 306Документ11 страницCase Study MKTG 306Yara100% (7)
- All India Hospital ListДокумент346 страницAll India Hospital ListGnanaSai DattatreyaОценок пока нет
- Ostra Psychiatry Case StudyДокумент4 страницыOstra Psychiatry Case StudyBatool Al-kharabsheh100% (2)
- Government College of Nursing Jodhpur (Raj.)Документ5 страницGovernment College of Nursing Jodhpur (Raj.)priyanka100% (1)
- NCP Knowledge DeficitДокумент2 страницыNCP Knowledge Deficitangeleigh viernesОценок пока нет
- Logo Express TaglineДокумент1 страницаLogo Express TaglineAbenkokehОценок пока нет
- Death To The Stock Photo - Photograph End User License (1-2014) PDFДокумент4 страницыDeath To The Stock Photo - Photograph End User License (1-2014) PDFAbenkokehОценок пока нет
- Kusman JANA362 17-04-11Документ10 страницKusman JANA362 17-04-11AbenkokehОценок пока нет
- Antono - AJIC 2010 - Letter To The Editor - RPRДокумент4 страницыAntono - AJIC 2010 - Letter To The Editor - RPRAbenkokehОценок пока нет
- Nelwan - TMIH 2010 - HIV HCV and HBV in Bandung Prison-1Документ8 страницNelwan - TMIH 2010 - HIV HCV and HBV in Bandung Prison-1AbenkokehОценок пока нет
- Seef Dental Clinic Bahrain - Dr. Sameh ShaheenДокумент1 страницаSeef Dental Clinic Bahrain - Dr. Sameh ShaheenMedicsindex Telepin Slidecase100% (3)
- Price List Update 1 April 2021-1Документ7 страницPrice List Update 1 April 2021-1Miliars IndotamaОценок пока нет
- Health and Safety Promotion: Healing For A Healthier Community: Healthcare ProgramДокумент4 страницыHealth and Safety Promotion: Healing For A Healthier Community: Healthcare ProgramFrancois MarcialОценок пока нет
- Clubbed Ques 2Документ19 страницClubbed Ques 2RadhakrishnanОценок пока нет
- Roles and Responsibilities of Pharmacy Staff Sample SOPДокумент9 страницRoles and Responsibilities of Pharmacy Staff Sample SOPjonaffe bantilanОценок пока нет
- Nellcor Khoury Clinical SummaryДокумент2 страницыNellcor Khoury Clinical SummaryjematheuОценок пока нет
- Maternal & Child Health CareДокумент51 страницаMaternal & Child Health CareBhumi ChouhanОценок пока нет
- 2022 February16 AnnexB EmergencyDepartmentPlanДокумент7 страниц2022 February16 AnnexB EmergencyDepartmentPlanJhasmin MejicaОценок пока нет
- Master Rotation Plan of Anm 2ND YearДокумент9 страницMaster Rotation Plan of Anm 2ND Yearkuruvagadda sagar50% (2)
- Term Paper Budget FinalДокумент24 страницыTerm Paper Budget FinalEshanth BalaОценок пока нет
- Tukimin SansuwitoДокумент2 страницыTukimin SansuwitoSahrudi RudiОценок пока нет
- CQC Standards Easy Format v2Документ29 страницCQC Standards Easy Format v2Simply Health and SafetyОценок пока нет
- Civic Drive, Filinvest City, Alabang 1781 Muntinlupa, PhilippinesДокумент18 страницCivic Drive, Filinvest City, Alabang 1781 Muntinlupa, Philippinesultimate_2226252Оценок пока нет
- JNM 21 414Документ9 страницJNM 21 414angelОценок пока нет
- Single Visit vs. Multiple Visits For Endodontic Treatment: A ReviewДокумент5 страницSingle Visit vs. Multiple Visits For Endodontic Treatment: A ReviewVi LinhОценок пока нет
- IDCRP Brown Bag Presentation - CRF - 26feb2015Документ33 страницыIDCRP Brown Bag Presentation - CRF - 26feb2015shivam singhОценок пока нет
- Advanced Postgraduate Diploma in HealthcareДокумент3 страницыAdvanced Postgraduate Diploma in HealthcarehaareetОценок пока нет
- New Century Health Clinic Ch.4Документ2 страницыNew Century Health Clinic Ch.4Natasha Rahman0% (2)
- MODULE I Definitivo - Optativa Enfermería 2019Документ18 страницMODULE I Definitivo - Optativa Enfermería 2019Dalbag Singh MahalОценок пока нет
- Pci FormsДокумент13 страницPci FormsKim SaludОценок пока нет
- Army Technical GuideДокумент27 страницArmy Technical GuideOlaniran Habib OlajideОценок пока нет
- 3 School Health Nursing - Field in NursingДокумент14 страниц3 School Health Nursing - Field in NursingsannsannОценок пока нет
- Drug Therapy ProblemДокумент19 страницDrug Therapy ProblemAulia NorfiantikaОценок пока нет