Вам также может понравиться
- Mastering ICU Nursing: A Quick Reference Guide, Interview Q&A, and TerminologyОт EverandMastering ICU Nursing: A Quick Reference Guide, Interview Q&A, and TerminologyОценок пока нет
- A Nurse's Guide to Caring for Cardiac Intervention PatientsОт EverandA Nurse's Guide to Caring for Cardiac Intervention PatientsОценок пока нет
- Icu OrientationДокумент9 страницIcu OrientationKshayna 1234Оценок пока нет
- Manual for Iv Therapy Procedures & Pain Management: Fourth EditionОт EverandManual for Iv Therapy Procedures & Pain Management: Fourth EditionОценок пока нет
- Welcome TO Intensive Care UnitДокумент42 страницыWelcome TO Intensive Care UnitKharene Lirazan100% (1)
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersОт EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersОценок пока нет
- ICU Orientation ManualДокумент107 страницICU Orientation Manualhery100% (2)
- Alfred Hosp ICU-orientation-manualДокумент85 страницAlfred Hosp ICU-orientation-manualdragon66Оценок пока нет
- A Nap with a Nurse Anesthetist: A Race Car AdventureОт EverandA Nap with a Nurse Anesthetist: A Race Car AdventureРейтинг: 4 из 5 звезд4/5 (1)
- Critical Care Nursing: Learning from PracticeОт EverandCritical Care Nursing: Learning from PracticeSuzanne BenchОценок пока нет
- ABC of Intensive CareДокумент49 страницABC of Intensive CareCurro MirallesОценок пока нет
- Kayla Holt - Graduate Nurse Cover LetterДокумент1 страницаKayla Holt - Graduate Nurse Cover Letterapi-353153135Оценок пока нет
- ICU ManagementДокумент26 страницICU Managementvamshidh100% (2)
- Ward-based Critical Care: a guide for health professionalsОт EverandWard-based Critical Care: a guide for health professionalsРейтинг: 4 из 5 звезд4/5 (5)
- 2 ICU Nursing For NoviceДокумент27 страниц2 ICU Nursing For NoviceChannelGОценок пока нет
- ICU ProceduresДокумент100 страницICU Proceduresvovaatanasov100% (1)
- How to Succeed New Graduate Nursing Job Interview & Bachelor of Nursing Clinical Placement?От EverandHow to Succeed New Graduate Nursing Job Interview & Bachelor of Nursing Clinical Placement?Оценок пока нет
- Increased Intracranial Pressure and Monitoring Site PDFДокумент21 страницаIncreased Intracranial Pressure and Monitoring Site PDFSari RakhmawatiОценок пока нет
- Critical Care/Intensive Care Unit Experience Internal Medicine INM.M INM.S CourseДокумент11 страницCritical Care/Intensive Care Unit Experience Internal Medicine INM.M INM.S CourseAmer Moh SarayrahОценок пока нет
- Acute Medical Emergencies: The Practical ApproachОт EverandAcute Medical Emergencies: The Practical ApproachОценок пока нет
- Learning IOM/HMD: Implications of the Institute of Medicine and Health & Medicine Division Reports for Nursing EducationОт EverandLearning IOM/HMD: Implications of the Institute of Medicine and Health & Medicine Division Reports for Nursing EducationРейтинг: 5 из 5 звезд5/5 (1)
- IcuДокумент8 страницIcuBikul Nayar100% (1)
- Manual IcuДокумент229 страницManual IcuMauricio PinneaparОценок пока нет
- Humanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperОт EverandHumanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperОценок пока нет
- Advanced Practice in Critical Care: A Case Study ApproachОт EverandAdvanced Practice in Critical Care: A Case Study ApproachSarah McGloinОценок пока нет
- Starting Out - New in The ICUДокумент30 страницStarting Out - New in The ICUashdmb217100% (1)
- Surviving the ICU: A Toolkit for the Critical Care NurseОт EverandSurviving the ICU: A Toolkit for the Critical Care NurseОценок пока нет
- ECMO Journal ClubДокумент15 страницECMO Journal Clubjoe kayongoОценок пока нет
- ICU Checklist - TEN FASTHUGSSS v3.0Документ35 страницICU Checklist - TEN FASTHUGSSS v3.0gxjjsjejdu100% (3)
- Invasive Hemodynamic MonitoringДокумент24 страницыInvasive Hemodynamic Monitoringheyyymeee100% (3)
- Assessment Algorithm For Sedated Adult ICU Patients: No YesДокумент18 страницAssessment Algorithm For Sedated Adult ICU Patients: No YeshendraОценок пока нет
- The Intensive Care Unit at The Mid Yorkshire Hospitals NHS TrustДокумент164 страницыThe Intensive Care Unit at The Mid Yorkshire Hospitals NHS TrustRajiv Srinivasa71% (7)
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationОт EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationРейтинг: 3 из 5 звезд3/5 (1)
- Pocket Tutor ECG Interpretation PDFДокумент165 страницPocket Tutor ECG Interpretation PDFasri100% (3)
- ICU Procedures ManualДокумент64 страницыICU Procedures Manualenumula kumar100% (1)
- Respiratory Therapy: 66 Test Questions Student Respiratory Therapists Get Wrong Every Time: (Volume 2 of 2): Now You Don't Have Too!: Respiratory Therapy Board Exam Preparation, #2От EverandRespiratory Therapy: 66 Test Questions Student Respiratory Therapists Get Wrong Every Time: (Volume 2 of 2): Now You Don't Have Too!: Respiratory Therapy Board Exam Preparation, #2Оценок пока нет
- Healthcare Environmental Services A Complete Guide - 2020 EditionОт EverandHealthcare Environmental Services A Complete Guide - 2020 EditionОценок пока нет
- 10MandatoryQI PDFДокумент10 страниц10MandatoryQI PDFEka BОценок пока нет
- WFICC Strategic Project SubmissionДокумент3 страницыWFICC Strategic Project SubmissionDadi VeenОценок пока нет
- PuzzlerДокумент9 страницPuzzlerDadi VeenОценок пока нет
- Student Hand Book For E-Learning ProgramДокумент9 страницStudent Hand Book For E-Learning ProgramDadi VeenОценок пока нет
- Gann's Square of Nine: by Jason SidneyДокумент6 страницGann's Square of Nine: by Jason SidneyDilip Valunj100% (1)
- Management of Trauma in ICUДокумент25 страницManagement of Trauma in ICUDadi VeenОценок пока нет
- ESPEN Guidelines On Nutrition in Acute Pancreatitis: Consensus StatementДокумент11 страницESPEN Guidelines On Nutrition in Acute Pancreatitis: Consensus StatementMemo HadyОценок пока нет
- 5 Moments For HHДокумент66 страниц5 Moments For HHtk100Оценок пока нет
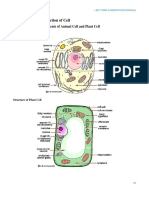
- BTE-308 L4 Tissue Culture Part III Tissue Culture MethodologyДокумент51 страницаBTE-308 L4 Tissue Culture Part III Tissue Culture MethodologyPURSUIT OF GROWTHОценок пока нет
- Airway Problems in PACUДокумент35 страницAirway Problems in PACUIndrani HemantkumarОценок пока нет
- ECG (Cardiology Clinic 2006)Документ127 страницECG (Cardiology Clinic 2006)VuqarОценок пока нет
- Carbon Cycle PDFДокумент9 страницCarbon Cycle PDFheyitsmemuahОценок пока нет
- Ecg MDДокумент121 страницаEcg MDdr. snehal patilОценок пока нет
- 86 Normal Low Tension Glaucoma PDFДокумент4 страницы86 Normal Low Tension Glaucoma PDFSherZalattha KuchikiElfОценок пока нет
- Loco For Cocoa 1 Running Head: LOCO FOR COCOAДокумент13 страницLoco For Cocoa 1 Running Head: LOCO FOR COCOAapi-310439970Оценок пока нет
- Per Dev Lesson For 1 WeekДокумент2 страницыPer Dev Lesson For 1 WeekEjay Balils IIОценок пока нет
- Simple AnatomyДокумент13 страницSimple AnatomyNicky DaymondОценок пока нет
- Chemical and Physical Properties of Nucleic AcidsДокумент6 страницChemical and Physical Properties of Nucleic AcidsSherlock Wesley ConanОценок пока нет
- Recognizing and Treating Breathing DisordersДокумент302 страницыRecognizing and Treating Breathing DisordersJun Kim100% (2)
- Communicating With A Sleeping PersonДокумент104 страницыCommunicating With A Sleeping PersonPeterMoranОценок пока нет
- LipidsДокумент16 страницLipidsEugene WongОценок пока нет
- PHARMACOLOGYДокумент36 страницPHARMACOLOGYjanr123456100% (1)
- 4 - Ditta - BIO173 - Unity of Life - 20204Документ13 страниц4 - Ditta - BIO173 - Unity of Life - 20204John ChoiОценок пока нет
- Consciousness And: Self-RegulafionДокумент461 страницаConsciousness And: Self-RegulafionderenifОценок пока нет
- Esthetics of Artificial GingivaДокумент13 страницEsthetics of Artificial GingivaSorabh JainОценок пока нет
- Residency: Called - To.See - Patient V1.1Документ111 страницResidency: Called - To.See - Patient V1.1Glen OngОценок пока нет
- Stages of LearningДокумент24 страницыStages of Learningapi-278802103Оценок пока нет
- Laboratory Tests of Thyroid Function - Uses and Limitations PDFДокумент16 страницLaboratory Tests of Thyroid Function - Uses and Limitations PDFMansouri HichemОценок пока нет
- Tactical BreathingДокумент3 страницыTactical Breathingsergio661204Оценок пока нет
- BS EN 00138-1994 (1995) Scan PDFДокумент24 страницыBS EN 00138-1994 (1995) Scan PDFShan Sandaruwan AbeywardeneОценок пока нет
- C - Syiam Amalia Rahmah - Topik 4Документ7 страницC - Syiam Amalia Rahmah - Topik 4Syiam Amalia RahmahОценок пока нет
- 083 41 Final Biologi T4 DLP-30-60Документ31 страница083 41 Final Biologi T4 DLP-30-60Farhan DarwisyОценок пока нет
- Stress Management Strategies Adopted by Teachers in Public Primary Schools in Obio/Akpor Local Government Area of Rivers State, Nigeria.Документ94 страницыStress Management Strategies Adopted by Teachers in Public Primary Schools in Obio/Akpor Local Government Area of Rivers State, Nigeria.sorbariОценок пока нет
- Brain Slides SEMINAR 1 - 220606 - 142811 - 220606 - 223805Документ32 страницыBrain Slides SEMINAR 1 - 220606 - 142811 - 220606 - 223805pang pangОценок пока нет
- Immediate Care of The NewbornДокумент12 страницImmediate Care of The NewbornLucilyn EbuengaОценок пока нет
- Lumbar Traction Review2Документ9 страницLumbar Traction Review2Phooi Yee LauОценок пока нет
- MR IntracranIal menIngIomas!!! Vazno!!!Документ5 страницMR IntracranIal menIngIomas!!! Vazno!!!StefanОценок пока нет