Вам также может понравиться
- Maxillofacial Prosthetics: Kamolphob Phasuk,, Steven P. HaugДокумент11 страницMaxillofacial Prosthetics: Kamolphob Phasuk,, Steven P. Hauglaura sanchez avilaОценок пока нет
- (2019) Cervical Margin Relocation - Case Series and New Classification Systems. CHECKДокумент13 страниц(2019) Cervical Margin Relocation - Case Series and New Classification Systems. CHECKBárbara Meza Lewis100% (1)
- Cosmetic Dentistry CSD 2013Документ3 страницыCosmetic Dentistry CSD 2013Rodrigo Daniel Vela RiveraОценок пока нет
- Deliperi S - PPAD - 2005 PDFДокумент9 страницDeliperi S - PPAD - 2005 PDFAlfredo PortocarreroОценок пока нет
- Rethinking FerruleДокумент10 страницRethinking FerruleteodudeОценок пока нет
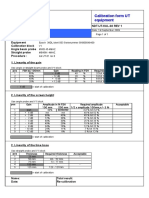
- Calibration Sheet Ultrasonic Test EquipmentДокумент1 страницаCalibration Sheet Ultrasonic Test EquipmentjohnОценок пока нет
- Endodontic Topics Volume 31 Issue 1 2014 (Doi 10.1111/etp.12066) Baba, Nadim Z. Goodacre, Charles J. - Restoration of Endodontically Treated Teeth - Contemporary Concepts andДокумент16 страницEndodontic Topics Volume 31 Issue 1 2014 (Doi 10.1111/etp.12066) Baba, Nadim Z. Goodacre, Charles J. - Restoration of Endodontically Treated Teeth - Contemporary Concepts andardeleanoana100% (1)
- Maciej Zarow Composite Veneers Vs Porcelain Veneers Which One To Choose Via WWW Styleitaliano OrgДокумент29 страницMaciej Zarow Composite Veneers Vs Porcelain Veneers Which One To Choose Via WWW Styleitaliano OrgghfhfdghОценок пока нет
- Evidence Based Management Third MolarsДокумент73 страницыEvidence Based Management Third MolarsCiutac ŞtefanОценок пока нет
- Inlay Onlay Parte 222 PDFДокумент23 страницыInlay Onlay Parte 222 PDFKhenny Jhynmir Paucar VillegasОценок пока нет
- The New Science of Strong TeethДокумент4 страницыThe New Science of Strong TeethThe Bioclear ClinicОценок пока нет
- Biomimetic (Latest)Документ127 страницBiomimetic (Latest)Pawee PiyasowanОценок пока нет
- Treatment Planning Single Maxillary Anterior Implants for DentistsОт EverandTreatment Planning Single Maxillary Anterior Implants for DentistsОценок пока нет
- Dan Lazar Workflow Composite Veneering On Non Vital Teeth ViaДокумент12 страницDan Lazar Workflow Composite Veneering On Non Vital Teeth Viaclaudia360Оценок пока нет
- Report Text About RainbowДокумент2 страницыReport Text About RainbowCornelia Ayu Trisna67% (3)
- The Single-Tooth RestorationДокумент5 страницThe Single-Tooth Restorationumerjaved86Оценок пока нет
- Shade MatchingДокумент6 страницShade MatchingdrsmritiОценок пока нет
- Additive Contour of Porcelain Veneers A Key Element in Enamel PreservationДокумент13 страницAdditive Contour of Porcelain Veneers A Key Element in Enamel PreservationPablo BenitezОценок пока нет
- 1 Cbct-Evaluation of Remaining Dentin Thickness and Fracture Resistance of Conventional and Conservative Access and Biomechanical Preparation in Molars Using Cone-beam Computed Tomography- An in Vitro StudyДокумент4 страницы1 Cbct-Evaluation of Remaining Dentin Thickness and Fracture Resistance of Conventional and Conservative Access and Biomechanical Preparation in Molars Using Cone-beam Computed Tomography- An in Vitro StudyalbertaugustineОценок пока нет
- Soumya S Jeena Profile BookДокумент53 страницыSoumya S Jeena Profile BooksoumyaОценок пока нет
- Posterior Composite Restoration UpdateДокумент10 страницPosterior Composite Restoration UpdateBianca IovoaiaОценок пока нет
- Etched Cast RestorationsДокумент41 страницаEtched Cast Restorationssharanya chekkarrajОценок пока нет
- Dentin Bonding Agents - An OverviewДокумент4 страницыDentin Bonding Agents - An OverviewIOSRjournalОценок пока нет
- Direct Cuspal-Coverage Posterior Resin Composite Restorations: A Case ReportДокумент8 страницDirect Cuspal-Coverage Posterior Resin Composite Restorations: A Case ReportDinar ArdhananeswariОценок пока нет
- Bioclear Posterior KitДокумент32 страницыBioclear Posterior KitSilvio DTОценок пока нет
- The Dahl Concept Past Present and FutureДокумент9 страницThe Dahl Concept Past Present and FuturevivigaitanОценок пока нет
- Avoiding and Treating Dental Complications: Best Practices in DentistryОт EverandAvoiding and Treating Dental Complications: Best Practices in DentistryDeborah A. TermeieОценок пока нет
- Form I-1 Centrifugal Pump Data SheetДокумент4 страницыForm I-1 Centrifugal Pump Data SheetJohnОценок пока нет
- Longair - Light and ColorДокумент38 страницLongair - Light and Colormordsith90Оценок пока нет
- Polishing Guide - DOTДокумент23 страницыPolishing Guide - DOTMeena Kulkarni100% (1)
- 3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFДокумент10 страниц3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFAnisha AnilОценок пока нет
- Journal of Prosthodontics on Dental ImplantsОт EverandJournal of Prosthodontics on Dental ImplantsAvinash BidraОценок пока нет
- Bonded Composites Versus Ceramic Veneers PDFДокумент7 страницBonded Composites Versus Ceramic Veneers PDFAnnaAffandieОценок пока нет
- Teflon Tape TechniqueДокумент6 страницTeflon Tape TechniqueJuan K. J. Shin100% (1)
- Posterior CompositeДокумент21 страницаPosterior CompositeNaji Z. ArandiОценок пока нет
- REVIEW - The Microtensile Bond TestДокумент12 страницREVIEW - The Microtensile Bond TestElmer Acevedo0% (1)
- Direct Posterior Restoration PDFДокумент14 страницDirect Posterior Restoration PDFياسر نادر حسين فليحОценок пока нет
- BIODENTINE EndovitalДокумент8 страницBIODENTINE EndovitalLupu SebastianОценок пока нет
- Vital Therapy in Carious ToothДокумент9 страницVital Therapy in Carious ToothAsh PeiОценок пока нет
- Challenges in dentin bondingДокумент11 страницChallenges in dentin bondingDanish SattarОценок пока нет
- Microbrush Stamp Technique To Achieve Occlusal Topography For Composite Resin Restorations - A Technical ReportДокумент7 страницMicrobrush Stamp Technique To Achieve Occlusal Topography For Composite Resin Restorations - A Technical ReportabulzОценок пока нет
- Implant Prosthetic DentistryДокумент86 страницImplant Prosthetic DentistryAnirban MallikОценок пока нет
- Bopt PanizДокумент9 страницBopt PanizIvan CarreraОценок пока нет
- Notes On Biological Considerations of Restorative DentistryДокумент5 страницNotes On Biological Considerations of Restorative DentistryTracie YWОценок пока нет
- Polyetheretherketone PEEK Dental Implants A Case FДокумент8 страницPolyetheretherketone PEEK Dental Implants A Case FPhoebe David100% (1)
- Class IV Composite Repair for Heavily Textured Central IncisorДокумент8 страницClass IV Composite Repair for Heavily Textured Central IncisorventynataliaОценок пока нет
- Smile Analysis What To MeasureДокумент6 страницSmile Analysis What To MeasureAli RazaОценок пока нет
- GingivectomyДокумент7 страницGingivectomyRirin SupriyaniОценок пока нет
- Review Peek PDFДокумент11 страницReview Peek PDFAlexandra Dumitrache100% (1)
- Bonnick - 2011 - Dental Clinics of North America PDFДокумент14 страницBonnick - 2011 - Dental Clinics of North America PDFKranti PrajapatiОценок пока нет
- Clinical Aids Manipulation of Rubber Dam Septa: An Aid To The Meticulous Isolation of Splinted ProsthesesДокумент4 страницыClinical Aids Manipulation of Rubber Dam Septa: An Aid To The Meticulous Isolation of Splinted ProsthesesAlfred Orozco100% (1)
- Bio Emulation Edinburgh EventsДокумент8 страницBio Emulation Edinburgh EventsAing MaungОценок пока нет
- Surgical Extrusion: A Dental TechniqueДокумент6 страницSurgical Extrusion: A Dental TechniqueDragos CiongaruОценок пока нет
- Recent Advances in Materials For All-Ceramic RestorationsДокумент19 страницRecent Advances in Materials For All-Ceramic RestorationsManishak YessayanОценок пока нет
- Preprosthetic and Reconstructive SurgeryДокумент32 страницыPreprosthetic and Reconstructive Surgeryruoiconmapu100% (1)
- Esthetic PostДокумент33 страницыEsthetic PostAhmed GendiaОценок пока нет
- Nixon Porcelain Veneer Kit II: Technique GuideДокумент6 страницNixon Porcelain Veneer Kit II: Technique GuideYuttapol PimpisonОценок пока нет
- Management of Discoloured ToothДокумент8 страницManagement of Discoloured ToothAnurtha AnuОценок пока нет
- Management of Peri-Implant Mucositis and Peri-Implantitis PDFДокумент19 страницManagement of Peri-Implant Mucositis and Peri-Implantitis PDFgirl33Оценок пока нет
- Topical Fluorides and Decalcification ArДокумент164 страницыTopical Fluorides and Decalcification ArArinaОценок пока нет
- Hall Technique, Stepwise Excavation, Partial Caries Removal TechniqueДокумент4 страницыHall Technique, Stepwise Excavation, Partial Caries Removal TechniqueImbador LiesiesОценок пока нет
- CPR For The Worn DentitionДокумент17 страницCPR For The Worn DentitionGustavo A OrtegonОценок пока нет
- Case Presentations & Online CEДокумент55 страницCase Presentations & Online CELeslie MorrowОценок пока нет
- The Properties and Selection of Posterior Direct RestorationsДокумент12 страницThe Properties and Selection of Posterior Direct RestorationsLeslie MorrowОценок пока нет
- Segmental Matrices For Primary and Permanent Class II Composite RestorationsДокумент2 страницыSegmental Matrices For Primary and Permanent Class II Composite RestorationsLeslie MorrowОценок пока нет
- Restoration of A Class II LesionДокумент9 страницRestoration of A Class II LesionLeslie MorrowОценок пока нет
- Clinical Solutions To Common Problems On Class II'sДокумент6 страницClinical Solutions To Common Problems On Class II'sLeslie MorrowОценок пока нет
- A Series of Photos Showing A MO Composite On #3Документ6 страницA Series of Photos Showing A MO Composite On #3Leslie MorrowОценок пока нет
- 3D Case Picture StudyДокумент5 страниц3D Case Picture StudyLeslie MorrowОценок пока нет
- 1 s2.0 S0020169309003971 MainДокумент8 страниц1 s2.0 S0020169309003971 MainusmanОценок пока нет
- What Is The Major Function of The Coating On An Arc Welding ElectrodeДокумент7 страницWhat Is The Major Function of The Coating On An Arc Welding ElectrodeElham Jaraine Garcia Lpt100% (4)
- OIL-Xplus Filtros Aire ComprimidoДокумент8 страницOIL-Xplus Filtros Aire ComprimidoMario Vazquez BОценок пока нет
- Nitocote ET402 : Constructive SolutionsДокумент4 страницыNitocote ET402 : Constructive Solutionsnoto.sugiartoОценок пока нет
- ARGUS ReportДокумент22 страницыARGUS ReportNguyễn Tường MinhОценок пока нет
- Third Order Elastic ConstantsДокумент3 страницыThird Order Elastic ConstantsElango PaulchamyОценок пока нет
- Validation of Raw MaterialДокумент22 страницыValidation of Raw MaterialPrima RamadhaniОценок пока нет
- 5-1-14 Recueil Methodes Vol 1 en 2012Документ488 страниц5-1-14 Recueil Methodes Vol 1 en 2012James Quynh NguyenОценок пока нет
- TPO Product CatalogДокумент210 страницTPO Product CatalogMiguel BrionesОценок пока нет
- Activity No. 2 The Microscope: Term FunctionДокумент5 страницActivity No. 2 The Microscope: Term FunctionUNSA MANEОценок пока нет
- Brewery Product Guide - FINAL 0619 PDFДокумент3 страницыBrewery Product Guide - FINAL 0619 PDFVictor LeiОценок пока нет
- Distillation Column Tray Selection & Sizing - 1 - Separation TechnologiesДокумент18 страницDistillation Column Tray Selection & Sizing - 1 - Separation TechnologiesOmesh Borole100% (1)
- Oxygen MSDS Safety GuideДокумент4 страницыOxygen MSDS Safety Guidelutfi_thalib3175Оценок пока нет
- Spectrophotometric Determination of The Equilibrium Constant of A Reaction DraftДокумент3 страницыSpectrophotometric Determination of The Equilibrium Constant of A Reaction DraftFem T. BartolomeОценок пока нет
- Assignment Inorganic ChemistryДокумент2 страницыAssignment Inorganic ChemistryRaquim Mondilo InventoОценок пока нет
- Resins Word DocumentДокумент8 страницResins Word DocumentHarish KakraniОценок пока нет
- Aalborg Solutions: Keep Your Feedwater Steaming HotДокумент2 страницыAalborg Solutions: Keep Your Feedwater Steaming HotRavikumar GangadharanОценок пока нет
- Acticide Bac 50 M MSDS PDFДокумент10 страницActicide Bac 50 M MSDS PDFmeОценок пока нет
- UHC Gen Chem 2 ManualДокумент67 страницUHC Gen Chem 2 ManualShumeng YangОценок пока нет
- Activity 2.2 Atomic Orbitals - S2-2015Документ10 страницActivity 2.2 Atomic Orbitals - S2-2015Devandra Eko RadityoОценок пока нет
- First Project ExamplesДокумент49 страницFirst Project ExamplesMeleti Meleti MeletiouОценок пока нет
- Oxidative WearДокумент17 страницOxidative WearManish Kumar SinghОценок пока нет
- Grade 12 Chemistry Activity SheetsДокумент6 страницGrade 12 Chemistry Activity SheetsKrizlyn MondalaОценок пока нет
- Chapter18 ThermoDynamicДокумент11 страницChapter18 ThermoDynamicVladimir MoroteОценок пока нет
- As Physics 2016Документ21 страницаAs Physics 2016WongXinXinОценок пока нет
- Determining Cation Exchange Capacity: A New Procedure For Calcareous and Gypsiferous SoilsДокумент5 страницDetermining Cation Exchange Capacity: A New Procedure For Calcareous and Gypsiferous SoilsM. Yusuf HermawanОценок пока нет