Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- CGHS empanelled hospitals and diagnostic centres in Delhi NCRДокумент76 страницCGHS empanelled hospitals and diagnostic centres in Delhi NCRJijo AbrahamОценок пока нет
- CGHS Approved Hospitals in HYDERABAD 2014Документ50 страницCGHS Approved Hospitals in HYDERABAD 2014Priyadarshini PearlОценок пока нет
- Bosch and Lomb FDA Submission DataДокумент31 страницаBosch and Lomb FDA Submission DataVinod RathoreОценок пока нет
- Capsular Bag Distension Syndrome Following Cataract Surgery JournalДокумент16 страницCapsular Bag Distension Syndrome Following Cataract Surgery Journalnaveen ratna KumarОценок пока нет
- 05 - Human Eye & The Colourful WorldДокумент26 страниц05 - Human Eye & The Colourful WorldAmogh Suman100% (2)
- Pinzas de Oftalmologia2 ASICO PDFДокумент231 страницаPinzas de Oftalmologia2 ASICO PDFKatty PaolaОценок пока нет
- Phacoemulsification & Extra Capsular Cataract ExtractionДокумент7 страницPhacoemulsification & Extra Capsular Cataract ExtractionJo-anne CorderoОценок пока нет
- Cmeseries 28Документ88 страницCmeseries 28ashishОценок пока нет
- Cataract Cataracts CataractДокумент6 страницCataract Cataracts Cataractta CОценок пока нет
- Medicsindex Egypt Member Profile DR Ahmad ElmassryДокумент9 страницMedicsindex Egypt Member Profile DR Ahmad ElmassryMedicsindex Telepin Slidecase100% (15)
- Senile Cataract (Age-Related Cataract) Treatment & Management - Medical Care, Surgical Care, ConsultationsДокумент5 страницSenile Cataract (Age-Related Cataract) Treatment & Management - Medical Care, Surgical Care, ConsultationsAhmad FahroziОценок пока нет
- Ultrasound BiomteryДокумент12 страницUltrasound BiomteryWillRoseroОценок пока нет
- Glaucoma and CataractДокумент30 страницGlaucoma and CataractJayselle ArvieОценок пока нет
- PresbiopiДокумент4 страницыPresbiopiapriyani ramahliaОценок пока нет
- Capsular Bag SulcusДокумент3 страницыCapsular Bag SulcusdrheriОценок пока нет
- Cghs Rates BangaloreДокумент26 страницCghs Rates Bangaloregr_viswanathОценок пока нет
- Design Input, Output and Verification DocumentДокумент30 страницDesign Input, Output and Verification DocumentHenry SpencerОценок пока нет
- Oculus: Pentacam Pentacam HRДокумент20 страницOculus: Pentacam Pentacam HRSaecio OpticoОценок пока нет
- AECS model for eradicating blindnessДокумент7 страницAECS model for eradicating blindnessShubha Brota RahaОценок пока нет
- Visual Acuity Outcome After Cataract SurgeryДокумент10 страницVisual Acuity Outcome After Cataract SurgeryAi AisyahОценок пока нет
- FC00909 VX130 Visionix en V2 PDFДокумент8 страницFC00909 VX130 Visionix en V2 PDFMarius CorneanuОценок пока нет
- Nylon LoopДокумент4 страницыNylon LooporlandgpicadoОценок пока нет
- Aravind Eye Hospital's Impactful Growth in IndiaДокумент6 страницAravind Eye Hospital's Impactful Growth in IndiaPrateek SinglaОценок пока нет
- Refractive Surgery PPP PDFДокумент75 страницRefractive Surgery PPP PDFdheerajkumarsahОценок пока нет
- Stallard's eye surgery pdf free download guideДокумент3 страницыStallard's eye surgery pdf free download guideCod Mobile100% (1)
- OS IOL Calculation OD: Lina Jati HardimanДокумент2 страницыOS IOL Calculation OD: Lina Jati HardimanFARMASI BEC BUBATОценок пока нет
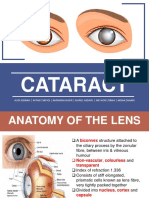
- Cataract: Audi Adibah - Affan Syafiqi - Amanina Nasir - Nurul Hidayu - Nik Nor Liyana - Arina ZahariДокумент57 страницCataract: Audi Adibah - Affan Syafiqi - Amanina Nasir - Nurul Hidayu - Nik Nor Liyana - Arina ZaharivictorssideОценок пока нет
- Acrysof IOL Prices2013 PDFДокумент2 страницыAcrysof IOL Prices2013 PDFedilefterОценок пока нет
- A Scan BiometryДокумент37 страницA Scan BiometryAnonymous Wb2LoZv9c100% (1)
- C11 P08 NPCBДокумент20 страницC11 P08 NPCBChandana KrishnaОценок пока нет