Вам также может понравиться
- Request For Mortgage Assistance (RMA) : Section 1: Borrower InformationДокумент7 страницRequest For Mortgage Assistance (RMA) : Section 1: Borrower InformationpeoniesОценок пока нет
- Application For Waiver or Deferral of FeesДокумент5 страницApplication For Waiver or Deferral of Feessbf20112011Оценок пока нет
- Dowddnload PDFLetterДокумент6 страницDowddnload PDFLettercmf318Оценок пока нет
- Teamster UPS Hardship FormДокумент19 страницTeamster UPS Hardship Formmnharris1550% (2)
- GEN1602Attach18450018SLDB UncДокумент2 страницыGEN1602Attach18450018SLDB UncjuandroaОценок пока нет
- 252-1 File 0Документ5 страниц252-1 File 0Sidharth KoulОценок пока нет
- Financial Information Sheet: Bal 1 Bal 2 TTLДокумент4 страницыFinancial Information Sheet: Bal 1 Bal 2 TTLSteve MontroseОценок пока нет
- Entire Packet 10Документ7 страницEntire Packet 10JohnnyLarsonОценок пока нет
- ClerkДокумент9 страницClerkPando DailyОценок пока нет
- Consumer Assistance Program Application: Receive Up To $1,500 To Retire Your VehicleДокумент0 страницConsumer Assistance Program Application: Receive Up To $1,500 To Retire Your VehicleNestor LopezОценок пока нет
- Recording Claim Losses and Expenses: Your Guide and Forms: OverviewДокумент11 страницRecording Claim Losses and Expenses: Your Guide and Forms: OverviewharryОценок пока нет
- Home Energy Assistance Universal Service Fund Weatherization AssistanceДокумент8 страницHome Energy Assistance Universal Service Fund Weatherization AssistanceChristian UlateОценок пока нет
- NY State Real Estate Broker Application - ForMДокумент3 страницыNY State Real Estate Broker Application - ForMmalter2991Оценок пока нет
- Personal Financial StatementДокумент3 страницыPersonal Financial StatementChristopher MacLeodОценок пока нет
- Request Restitution FormДокумент2 страницыRequest Restitution Formjlori82Оценок пока нет
- 401 KhardshipДокумент10 страниц401 KhardshipRickey LemonsОценок пока нет
- Emergency Fund Assistance Application FinalДокумент1 страницаEmergency Fund Assistance Application Finalapi-278611763Оценок пока нет
- Disaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsОт EverandDisaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsОценок пока нет
- L1 L9 Application Information UpdateДокумент3 страницыL1 L9 Application Information UpdateCody GroseОценок пока нет
- Request For Change of Program or Place of Training: Part I - Identification and Personal Information Va Date StampДокумент4 страницыRequest For Change of Program or Place of Training: Part I - Identification and Personal Information Va Date StampVictorRosaОценок пока нет
- CitiMortgage hardship applicationДокумент4 страницыCitiMortgage hardship applicationRob SmithОценок пока нет
- Binder Materials Legal Issues in Time of DisasterДокумент36 страницBinder Materials Legal Issues in Time of DisasterkitkatchaiosОценок пока нет
- Indigency Application (Completed) PDFДокумент4 страницыIndigency Application (Completed) PDFdcarson90Оценок пока нет
- Rose Hudson Workbook Case StudyДокумент6 страницRose Hudson Workbook Case StudyMary O'KeeffeОценок пока нет
- Fema Appeal Template 3Документ6 страницFema Appeal Template 3api-32792506772% (18)
- Chase Loan Modification PacketДокумент11 страницChase Loan Modification PacketSince 1990 BK AND MOTIONS AT YAHOO COM100% (1)
- Bankruptcy QuestionnaireДокумент7 страницBankruptcy QuestionnaireArasto FarsadОценок пока нет
- LPA120 Fees Exemptions RemissionsДокумент4 страницыLPA120 Fees Exemptions RemissionssriharshamysuruОценок пока нет
- Instructions To Guardian:: Guardian'S Report - Minor Current Reporting Period From - ToДокумент5 страницInstructions To Guardian:: Guardian'S Report - Minor Current Reporting Period From - ToLaurena ThompsonОценок пока нет
- NYSMAP ApplicationДокумент14 страницNYSMAP ApplicationChacheiОценок пока нет
- Pratap Asset and Liabilities AffidavitДокумент15 страницPratap Asset and Liabilities Affidavitraju yadavОценок пока нет
- Application Checklist - NationalДокумент1 страницаApplication Checklist - NationalindianluverОценок пока нет
- Mortgage Assistance Application Uniform Applicant Assistance Form / Form 710Документ9 страницMortgage Assistance Application Uniform Applicant Assistance Form / Form 710Danton LawsonОценок пока нет
- SG 402 Hardship Cert FormДокумент4 страницыSG 402 Hardship Cert FormKendal CliffordОценок пока нет
- Uniform Residential Loan Application: I. Type of Mortgage and Terms of LoanДокумент5 страницUniform Residential Loan Application: I. Type of Mortgage and Terms of LoanSean ObrienОценок пока нет
- Loan Number: Borrower Co-BorrowerДокумент5 страницLoan Number: Borrower Co-BorrowerJeff BettsОценок пока нет
- Acton ERAP Application Final Draft 30aug2021 - 202109071701563558Документ7 страницActon ERAP Application Final Draft 30aug2021 - 202109071701563558J&A Partners JANОценок пока нет
- Mortgage App Form 1003Документ5 страницMortgage App Form 1003api-305651288Оценок пока нет
- Financial Assistance Scheme For Uncontracted Assessors: Application Form - IndividualsДокумент4 страницыFinancial Assistance Scheme For Uncontracted Assessors: Application Form - Individualsn_san5Оценок пока нет
- Employee Hardship Fund Grant ApplicationДокумент2 страницыEmployee Hardship Fund Grant Application_clinton100% (2)
- MOTION To Request To Waive Court Fees in California Civil CourtДокумент2 страницыMOTION To Request To Waive Court Fees in California Civil Courtsfsu1997Оценок пока нет
- Kimberley Hoff PAR 117 Jdf11091 Temporary Orders AgreementДокумент4 страницыKimberley Hoff PAR 117 Jdf11091 Temporary Orders AgreementlegalparaeagleОценок пока нет
- 2015 Uc Health FaaДокумент4 страницы2015 Uc Health Faaapi-263913260Оценок пока нет
- Blank 1003Документ4 страницыBlank 1003api-296319445Оценок пока нет
- Tenant Evaluation FormДокумент4 страницыTenant Evaluation FormLux's TerminalОценок пока нет
- CD 9600Документ6 страницCD 9600api-2812926660% (1)
- Date: - Application #Документ4 страницыDate: - Application #988965Оценок пока нет
- Annual Application: GSB MBA Nonprofit/Public Service Loan Forgiveness ProgramДокумент7 страницAnnual Application: GSB MBA Nonprofit/Public Service Loan Forgiveness ProgramSunil PanwarОценок пока нет
- Uniform Residential Loan Application: I. Type of Mortgage and Terms of LoanДокумент13 страницUniform Residential Loan Application: I. Type of Mortgage and Terms of Loanmalinda_haneyОценок пока нет
- Hud Add A Household Member Checklist: Return All Original Forms in The Order of The ChecklistДокумент1 страницаHud Add A Household Member Checklist: Return All Original Forms in The Order of The ChecklistAchraf AaRôchêОценок пока нет
- Indigency Application (Blank) PDFДокумент3 страницыIndigency Application (Blank) PDFdcarson90Оценок пока нет
- Commercial - Loan - Application PDFДокумент4 страницыCommercial - Loan - Application PDFKent WhiteОценок пока нет
- CS - Man - 200 CHILD SUPPORT ENFORCEMENT MANUAL CHAPTER II CASE PROCESSINGДокумент104 страницыCS - Man - 200 CHILD SUPPORT ENFORCEMENT MANUAL CHAPTER II CASE PROCESSINGLisa Stinocher OHanlonОценок пока нет
- Traffic TRL I93Документ2 страницыTraffic TRL I93ciejhae3111Оценок пока нет
- Interactive 1003Документ3 страницыInteractive 1003bradley_germainОценок пока нет
- Description: Tags: GEN0205DДокумент2 страницыDescription: Tags: GEN0205Danon-4443Оценок пока нет
- Form W 10Документ7 страницForm W 10zigzag7842611Оценок пока нет
- HM Government: Security Appraisal FormДокумент15 страницHM Government: Security Appraisal FormFBОценок пока нет
- How To File Your Own Bankruptcy: The Step-by-Step Handbook to Filing Your Own Bankruptcy PetitionОт EverandHow To File Your Own Bankruptcy: The Step-by-Step Handbook to Filing Your Own Bankruptcy PetitionОценок пока нет
- 2017 Alabama Poverty Data SheetДокумент2 страницы2017 Alabama Poverty Data SheetAlabama Possible100% (1)
- 2016 Alabama Poverty Data SheetДокумент2 страницы2016 Alabama Poverty Data SheetAlabama Possible100% (7)
- 2014 Alabama Possible 990Документ39 страниц2014 Alabama Possible 990Alabama PossibleОценок пока нет
- 2015 Data SheetДокумент2 страницы2015 Data SheetAlabama Possible100% (2)
- 2014 Lifetime of Learning RegistrationДокумент1 страница2014 Lifetime of Learning RegistrationAlabama PossibleОценок пока нет
- Alabama Possible Operations DirectorДокумент3 страницыAlabama Possible Operations DirectorAlabama PossibleОценок пока нет
- Alabama Possible's 2015 Annual ReportДокумент4 страницыAlabama Possible's 2015 Annual ReportAlabama PossibleОценок пока нет
- 2015 Alabama Possible College Access and Success Impact ReportДокумент12 страниц2015 Alabama Possible College Access and Success Impact ReportAlabama PossibleОценок пока нет
- 2015 Benefit Dinner Ticket FormДокумент1 страница2015 Benefit Dinner Ticket FormAlabama PossibleОценок пока нет
- 2015 Benefit Dinner Ticket FormДокумент1 страница2015 Benefit Dinner Ticket FormAlabama PossibleОценок пока нет
- 2014 Blueprints College Access Initative Impact ReportДокумент8 страниц2014 Blueprints College Access Initative Impact ReportAlabama PossibleОценок пока нет
- 2014 Benefit Dinner Ticket FormДокумент1 страница2014 Benefit Dinner Ticket FormAlabama PossibleОценок пока нет
- Blueprints MLK Day College FairДокумент1 страницаBlueprints MLK Day College FairAlabama PossibleОценок пока нет
- 2013 Advocacy WorkshopДокумент1 страница2013 Advocacy WorkshopAlabama PossibleОценок пока нет
- Lifetime of Learning: Bill Muse, PHDДокумент2 страницыLifetime of Learning: Bill Muse, PHDAlabama PossibleОценок пока нет
- White Privilege: Unpacking The Invisible KnapsackДокумент2 страницыWhite Privilege: Unpacking The Invisible KnapsackAlabama PossibleОценок пока нет
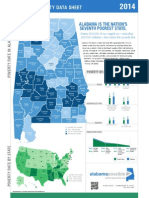
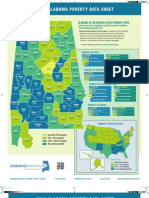
- 2014 Alabama Possible Poverty Data SheetДокумент2 страницы2014 Alabama Possible Poverty Data SheetAlabama PossibleОценок пока нет
- Alabama Possible-Alabama Poverty Project 20th Anniversary Sponsor PackageДокумент7 страницAlabama Possible-Alabama Poverty Project 20th Anniversary Sponsor PackageAlabama PossibleОценок пока нет
- Alabama Possible - Annual Lifetime of Learning ConferenceДокумент20 страницAlabama Possible - Annual Lifetime of Learning ConferenceAlabama PossibleОценок пока нет
- A Summit On Civic Engagement and Alabama's Two Year Colleges Engaging Alabama Communities Through Two-Year Colleges: Real Learning, Real ChangeДокумент1 страницаA Summit On Civic Engagement and Alabama's Two Year Colleges Engaging Alabama Communities Through Two-Year Colleges: Real Learning, Real ChangeKristina ScottОценок пока нет
- 2012 Food Security Fact SheetДокумент1 страница2012 Food Security Fact SheetAlabama PossibleОценок пока нет
- 2013 Alabama Poverty Data SheetДокумент2 страницы2013 Alabama Poverty Data SheetAlabama PossibleОценок пока нет
- What We Don't Talk About When We Talk About ServiceДокумент7 страницWhat We Don't Talk About When We Talk About ServiceAlabama PossibleОценок пока нет
- Partnering With The Homeless CoalitionДокумент19 страницPartnering With The Homeless CoalitionAlabama PossibleОценок пока нет
- The Economic Impact of Undocumented Workers in A Culture of Competition: Separating Truth From MythДокумент2 страницыThe Economic Impact of Undocumented Workers in A Culture of Competition: Separating Truth From MythAlabama PossibleОценок пока нет
- Reading Micro and Macro Level Structures and Contexts WorksheetДокумент1 страницаReading Micro and Macro Level Structures and Contexts WorksheetAlabama PossibleОценок пока нет
- Shoal Creek Prentice Village - University of MontevalloДокумент2 страницыShoal Creek Prentice Village - University of MontevalloAlabama PossibleОценок пока нет
- Spirituality Marginalization ChartДокумент1 страницаSpirituality Marginalization ChartAlabama PossibleОценок пока нет
- Reflecting On Self and Other WorksheetДокумент1 страницаReflecting On Self and Other WorksheetAlabama PossibleОценок пока нет
- 2012 Lifetime of Learning AgendaДокумент3 страницы2012 Lifetime of Learning AgendaAlabama PossibleОценок пока нет
- Bluetooth Home Automation Using ArduinoДокумент25 страницBluetooth Home Automation Using ArduinoRabiОценок пока нет
- Practice Like-Love - Hate and PronounsДокумент3 страницыPractice Like-Love - Hate and PronounsangelinarojascnОценок пока нет
- National Advisory Committee For AeronauticsДокумент36 страницNational Advisory Committee For AeronauticsSamuel ChristioОценок пока нет
- WassiДокумент12 страницWassiwaseem0808Оценок пока нет
- Postnatal Assessment: Name Date: Age: D.O.A: Sex: Hospital: Marital Status: IP .NoДокумент11 страницPostnatal Assessment: Name Date: Age: D.O.A: Sex: Hospital: Marital Status: IP .NoRadha SriОценок пока нет
- Ana White - PLANS - A Murphy Bed YOU Can Build, and Afford To Build - 2011-03-03Документ20 страницAna White - PLANS - A Murphy Bed YOU Can Build, and Afford To Build - 2011-03-03Ahmad KamilОценок пока нет
- Corn MillingДокумент4 страницыCorn Millingonetwoone s50% (1)
- Board 2Документ1 страницаBoard 2kristine_nilsen_2Оценок пока нет
- Fong vs. DueñasДокумент2 страницыFong vs. DueñasWinter Woods100% (3)
- Device Interface Device Type (Router, Switch, Host) IP Address Subnet Mask Default GatewayДокумент2 страницыDevice Interface Device Type (Router, Switch, Host) IP Address Subnet Mask Default GatewayRohit Chouhan0% (1)
- Your Inquiry EPALISPM Euro PalletsДокумент3 страницыYour Inquiry EPALISPM Euro PalletsChristopher EvansОценок пока нет
- TransistorДокумент1 страницаTransistorXhaОценок пока нет
- Restructuring Egypt's Railways - Augst 05 PDFДокумент28 страницRestructuring Egypt's Railways - Augst 05 PDFMahmoud Abo-hashemОценок пока нет
- Biomotor Development For Speed-Power Athletes: Mike Young, PHD Whitecaps FC - Vancouver, BC Athletic Lab - Cary, NCДокумент125 страницBiomotor Development For Speed-Power Athletes: Mike Young, PHD Whitecaps FC - Vancouver, BC Athletic Lab - Cary, NCAlpesh Jadhav100% (1)
- Driving Continuous Improvement by Developing and Leveraging Lean Key Performance IndicatorsДокумент10 страницDriving Continuous Improvement by Developing and Leveraging Lean Key Performance IndicatorskellendadОценок пока нет
- Russian Tea Market Growth and Brand PreferenceДокумент6 страницRussian Tea Market Growth and Brand PreferenceKing KhanОценок пока нет
- ASTM D256-10 - Standard Test Methods For Determining The Izod Pendulum Impact Resistance of PlasticsДокумент20 страницASTM D256-10 - Standard Test Methods For Determining The Izod Pendulum Impact Resistance of PlasticsEng. Emílio DechenОценок пока нет
- Piping MaterialДокумент45 страницPiping MaterialLcm TnlОценок пока нет
- Practical Research 2: Self-Learning PackageДокумент3 страницыPractical Research 2: Self-Learning PackagePrinces BaccayОценок пока нет
- Machine Spindle Noses: 6 Bison - Bial S. AДокумент2 страницыMachine Spindle Noses: 6 Bison - Bial S. AshanehatfieldОценок пока нет
- NPV Irr ArrДокумент16 страницNPV Irr ArrAnjaliОценок пока нет
- Budget ControlДокумент7 страницBudget ControlArnel CopinaОценок пока нет
- Steps To Configure Linux For Oracle 9i Installation: 1. Change Kernel ParametersДокумент5 страницSteps To Configure Linux For Oracle 9i Installation: 1. Change Kernel ParametersruhelanikОценок пока нет
- Exor EPF-1032 DatasheetДокумент2 страницыExor EPF-1032 DatasheetElectromateОценок пока нет
- Lecture 1 Family PlanningДокумент84 страницыLecture 1 Family PlanningAlfie Adam Ramillano100% (4)
- Post Marketing SurveillanceДокумент19 страницPost Marketing SurveillanceRamanjeet SinghОценок пока нет
- Ecole Polytechnique Federale de LausanneДокумент44 страницыEcole Polytechnique Federale de LausanneSyed Yahya HussainОценок пока нет
- Transformer Oil Testing MethodsДокумент10 страницTransformer Oil Testing MethodsDEE TOTLVJAОценок пока нет
- 2.4 Avogadro's Hypothesis+ Equivalent MassesДокумент12 страниц2.4 Avogadro's Hypothesis+ Equivalent MassesSantosh MandalОценок пока нет
- 2019-10 Best Practices For Ovirt Backup and Recovery PDFДокумент33 страницы2019-10 Best Practices For Ovirt Backup and Recovery PDFAntonius SonyОценок пока нет