Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Unilever BD Recruitment and Selection ProcessДокумент34 страницыUnilever BD Recruitment and Selection Processacidreign100% (1)
- HR Activity in Nissan CompanyДокумент6 страницHR Activity in Nissan CompanyAnnapurna VinjamuriОценок пока нет
- SWOT AnalysisДокумент6 страницSWOT AnalysisAli Najaf NaqviОценок пока нет
- Labor Economics 7Th Edition George Borjas Solutions Manual Full Chapter PDFДокумент34 страницыLabor Economics 7Th Edition George Borjas Solutions Manual Full Chapter PDFphualexandrad3992% (12)
- CONSTITUTION of The Ghana Tourism Federation-GHATOF-SPD'NBW-Jean Lukaz Edit-DeC 07-2009Документ25 страницCONSTITUTION of The Ghana Tourism Federation-GHATOF-SPD'NBW-Jean Lukaz Edit-DeC 07-2009Jean Lukaz100% (1)
- Karnataka Minimum Wages For The Year 2021Документ1 страницаKarnataka Minimum Wages For The Year 2021Anusree RoyОценок пока нет
- Monster Resume SearchДокумент8 страницMonster Resume Searchgt7gb636100% (1)
- Class Xii Compiled by Sudhir Sinha Business StudiesДокумент7 страницClass Xii Compiled by Sudhir Sinha Business StudiesSudhir SinhaОценок пока нет
- PromissoryДокумент1 страницаPromissoryDiyames RamosОценок пока нет
- HotsДокумент46 страницHotsTina Roy100% (1)
- Spousal Work Permit Tutorial June 1Документ2 страницыSpousal Work Permit Tutorial June 1sureshkanna2Оценок пока нет
- AI in HR A Conceptual FrameworkДокумент4 страницыAI in HR A Conceptual FrameworkAbeeth SОценок пока нет
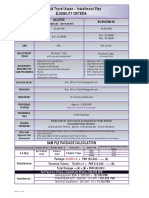
- Labbaik Travel Asaan - Installment Plan Eligibility CriteriaДокумент1 страницаLabbaik Travel Asaan - Installment Plan Eligibility CriteriamuhammadTzОценок пока нет
- Nando's Final UniДокумент27 страницNando's Final Uniamna186Оценок пока нет
- Introduction of Apple. Inc.: (Nature and Experiences)Документ11 страницIntroduction of Apple. Inc.: (Nature and Experiences)Vi AtilanoОценок пока нет
- Job Description: King's College King's Parade Cambridge CB2 1STДокумент3 страницыJob Description: King's College King's Parade Cambridge CB2 1STsiva8000Оценок пока нет
- Ableism in Deaf Community We Are of A Different ClassДокумент17 страницAbleism in Deaf Community We Are of A Different Classapi-319843117Оценок пока нет
- Guest Lecture On PmsДокумент12 страницGuest Lecture On PmsAshrazorОценок пока нет
- Nike SweatshopsДокумент5 страницNike SweatshopsMichelle I. Smith0% (1)
- FIDIC ImpДокумент60 страницFIDIC ImpSajad WaniОценок пока нет
- "Job Satisfaction": "Apollo Hospitals" VisakhapatnamДокумент91 страница"Job Satisfaction": "Apollo Hospitals" Visakhapatnamdeva kiranОценок пока нет
- Ideology and Methodology Duncan FoleyДокумент11 страницIdeology and Methodology Duncan Foley신재석Оценок пока нет
- MNIT Resume StructureДокумент3 страницыMNIT Resume StructurePrabhaMeenaОценок пока нет
- Doctrine of Piercing The Corporate Veil - Case DigestДокумент2 страницыDoctrine of Piercing The Corporate Veil - Case DigestlookalikenilongОценок пока нет
- 8 Signs of A Toxic LeaderДокумент11 страниц8 Signs of A Toxic Leaderdragonxyz70Оценок пока нет
- Ipcr BCCДокумент3 страницыIpcr BCCAnjo EllisОценок пока нет
- Medical Center Sues Former COO For Stealing Information - Southeast Texas RecordДокумент2 страницыMedical Center Sues Former COO For Stealing Information - Southeast Texas RecorddocinformerОценок пока нет
- HandBook VoluntaryRetirementДокумент2 страницыHandBook VoluntaryRetirementJgun Commentator JaganОценок пока нет
- DMIC TenderДокумент96 страницDMIC TenderAnkesh KhonaОценок пока нет
- Management: Delegation and Stages of Team DevelopmentДокумент76 страницManagement: Delegation and Stages of Team DevelopmentAlvin OroscoОценок пока нет