Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Form 2 Notes-1Документ53 страницыForm 2 Notes-1William NjorogeОценок пока нет
- Pulse Flour From Wheat MillerДокумент23 страницыPulse Flour From Wheat MillerCao Trọng HiếuОценок пока нет
- Staar Eoc 2016test Bio F 7Документ39 страницStaar Eoc 2016test Bio F 7api-293216402Оценок пока нет
- Study Guide Cardio Tayang by Gextha 30 Maret 2015Документ82 страницыStudy Guide Cardio Tayang by Gextha 30 Maret 2015Adi ParamarthaОценок пока нет
- Short Note Biology Form 5-Chapter 3 Coordination and ResponseДокумент6 страницShort Note Biology Form 5-Chapter 3 Coordination and Responsesalamah_sabri75% (4)
- Approved LaboratoriesДокумент22 страницыApproved LaboratoriesPaul CОценок пока нет
- Pharyngeal ArchesДокумент35 страницPharyngeal ArchesconstantinilieОценок пока нет
- Social IntelligenceДокумент10 страницSocial IntelligencePeterMarquezОценок пока нет
- The Truth About Honey - White Paper PDFДокумент5 страницThe Truth About Honey - White Paper PDFSergio PérezОценок пока нет
- Kimia Daun PandanДокумент4 страницыKimia Daun Pandanlutfi_alhayathullahОценок пока нет
- EuglenidДокумент4 страницыEuglenidx456456456xОценок пока нет
- Aims Stress - The SeedДокумент27 страницAims Stress - The SeedFx KovacsОценок пока нет
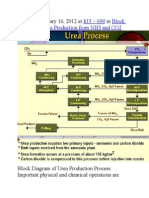
- Published January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2Документ9 страницPublished January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2himanshuchawla654Оценок пока нет
- AquaLab ManualДокумент123 страницыAquaLab ManualBrent WilsonОценок пока нет
- CLS Aipmt 15 16 XIII Zoo Study Package 2 Set 1 Chapter 3Документ30 страницCLS Aipmt 15 16 XIII Zoo Study Package 2 Set 1 Chapter 3Santu Karmakar100% (1)
- Gen. Zoo. Final ReviewerДокумент34 страницыGen. Zoo. Final ReviewerAshley FranciscoОценок пока нет
- L&M ResearchДокумент145 страницL&M ResearchJulia PurperaОценок пока нет
- Chauhan2017mulberry SericultureДокумент67 страницChauhan2017mulberry SericultureNarasimha Murthy S VОценок пока нет
- Escueoloside A2 From TomatoДокумент8 страницEscueoloside A2 From TomatoShyam ReddyОценок пока нет
- Qualitative and QuantitativeДокумент2 страницыQualitative and Quantitativetimmierivera100% (1)
- "Material Ecocriticism and The Creativity of Storied Matter" by Serpil OppermannДокумент16 страниц"Material Ecocriticism and The Creativity of Storied Matter" by Serpil OppermannoppermanОценок пока нет
- Chapter 1Документ4 страницыChapter 1Nikoleta RudnikОценок пока нет
- Accessory Organ of The AbdomenДокумент58 страницAccessory Organ of The AbdomenOgundipe olorunfemiОценок пока нет
- Blood Doping PPT PresentationДокумент26 страницBlood Doping PPT Presentationee4254100% (1)
- Allen and Hightower Population Dynamics Chapter IFM3Документ38 страницAllen and Hightower Population Dynamics Chapter IFM3Emily HaugОценок пока нет
- On The Nature of The Symbiotic Man in Joël de RosnayДокумент12 страницOn The Nature of The Symbiotic Man in Joël de RosnayAJHSSR JournalОценок пока нет
- Capsicum Annuum L., Commonly Known As Hot Pepper or Chilli Is AДокумент11 страницCapsicum Annuum L., Commonly Known As Hot Pepper or Chilli Is Ajavedsaqi100% (1)
- Taxonomy of Haematococcus PluvialisДокумент2 страницыTaxonomy of Haematococcus PluvialisKomathi BalasupramaniamОценок пока нет
- Artikel SkripsiДокумент12 страницArtikel SkripsiSari RofiqohОценок пока нет
- USAID BD Handbook Oct 2015 508Документ280 страницUSAID BD Handbook Oct 2015 508vasconcelos1322Оценок пока нет