Вам также может понравиться
- DengueДокумент14 страницDengueKarenn Joy Concepcion OctubreОценок пока нет
- NCP DengueДокумент4 страницыNCP DengueJanna Carrel Isabedra Rodio100% (2)
- NCP For Dengue Hemorrhagic FeverДокумент14 страницNCP For Dengue Hemorrhagic FeverKim Celeste Matulac100% (3)
- NCP-Dengue Hemorrhagic FeverДокумент8 страницNCP-Dengue Hemorrhagic Feverjunrey1990Оценок пока нет
- Planning (Nursing Care Plans)Документ14 страницPlanning (Nursing Care Plans)plumhie100% (1)
- NCP DengueДокумент3 страницыNCP DengueRichmund Earl Geron100% (1)
- NCP For DengueДокумент6 страницNCP For DengueSoniaMarieBalanayОценок пока нет
- NCP DengueДокумент3 страницыNCP DengueYeana Alon50% (4)
- Dengue NCP PediaДокумент3 страницыDengue NCP Pediaraven riveraОценок пока нет
- DIAGNOSIS Hyperthermia Related To Increased Metabolic Rate, Illness. ASSESSMENT SubjectiveДокумент1 страницаDIAGNOSIS Hyperthermia Related To Increased Metabolic Rate, Illness. ASSESSMENT Subjectivemawel100% (1)
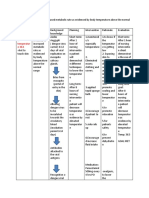
- VI. Nursing Care Plan Cues Nursing Diagnosis Analysis Goals and Objectives Intervention Rationale EvaluationДокумент3 страницыVI. Nursing Care Plan Cues Nursing Diagnosis Analysis Goals and Objectives Intervention Rationale EvaluationJenny AjocОценок пока нет
- NCP Baby DДокумент3 страницыNCP Baby DYna LafuenteОценок пока нет
- Deficit)Документ2 страницыDeficit)Lee DeeОценок пока нет
- Discharge Plan For Dengue Fever 1Документ4 страницыDischarge Plan For Dengue Fever 1Cecille Ursua0% (1)
- NCP UtiДокумент1 страницаNCP UtiElaisa Mae Delos SantosОценок пока нет
- HyperthermiaДокумент6 страницHyperthermiaBerlyn FelicianoОценок пока нет
- Nursing Care Plan Risk For InjuryДокумент1 страницаNursing Care Plan Risk For InjuryAce Dioso TubascoОценок пока нет
- NCP GastroenteritisДокумент1 страницаNCP GastroenteritisFranchesca PaunganОценок пока нет
- NCP DengueДокумент4 страницыNCP DengueAriaОценок пока нет
- NCP DengueДокумент8 страницNCP Dengueelaine_tengco50% (2)
- NCP Micu Hascvd Cad - RioДокумент5 страницNCP Micu Hascvd Cad - RioRio BonifacioОценок пока нет
- Deficient Fluid Volume (Vanene)Документ7 страницDeficient Fluid Volume (Vanene)jajalerОценок пока нет
- NCP HyperthermiaДокумент6 страницNCP HyperthermiaGrax DeeОценок пока нет
- NCP For DengueДокумент1 страницаNCP For DengueyelbonifacioОценок пока нет
- F-DAR For Pain: RelaxationДокумент4 страницыF-DAR For Pain: RelaxationjaypeeОценок пока нет
- Nursing Care Plan For Dengue Hemmorrhagic FeverДокумент6 страницNursing Care Plan For Dengue Hemmorrhagic FeverMean Elepaño100% (1)
- NCP HyperthermiaДокумент1 страницаNCP HyperthermiaPatricia Trinidad100% (1)
- Impaired Skin IntegrityДокумент3 страницыImpaired Skin IntegrityAubrey SungaОценок пока нет
- Nursing Care Plan Risk For Infection OB University of Santo Tomas College of NursingДокумент2 страницыNursing Care Plan Risk For Infection OB University of Santo Tomas College of NursingKaren ValdezОценок пока нет
- Patient's Name: Date of Admission: Age: Physician: Religion: Diagnosis: Nationality: Diet: Room and Bed No.Документ4 страницыPatient's Name: Date of Admission: Age: Physician: Religion: Diagnosis: Nationality: Diet: Room and Bed No.rammyestellaОценок пока нет
- Fluid Volume DeficitДокумент2 страницыFluid Volume DeficitRuby AnneОценок пока нет
- NCP and Fdar Wk2 Sarscov-19Документ4 страницыNCP and Fdar Wk2 Sarscov-19Jamaica Malicdem0% (1)
- Dengue NCP (Risk For Bleeding)Документ5 страницDengue NCP (Risk For Bleeding)Bernadette Malamug50% (6)
- Subjective Cues: Ineffective Tissue PerfusionДокумент3 страницыSubjective Cues: Ineffective Tissue PerfusionFlorence Lacea Rotsap-DeguitОценок пока нет
- NCP Dengue Fever Hyperthermia and Acute PainДокумент4 страницыNCP Dengue Fever Hyperthermia and Acute PainJordz PlaciОценок пока нет
- Geria NCPДокумент4 страницыGeria NCPBrylle CapiliОценок пока нет
- 3 Nursing Care Plans For Dengue Hemorrhagic FeverДокумент8 страниц3 Nursing Care Plans For Dengue Hemorrhagic FeverCarren Wingwash100% (3)
- Name of DrugДокумент6 страницName of Drug私 シャーロット100% (1)
- NCP Gastritis NewДокумент3 страницыNCP Gastritis NewNova Triska Purnama Sari0% (1)
- NCP DengueДокумент4 страницыNCP Denguesarzlasco0980% (5)
- Nursing Care Plan Student Nurse: Diestro, Angela Mae BSN 2BДокумент3 страницыNursing Care Plan Student Nurse: Diestro, Angela Mae BSN 2BAngela Mae DiestroОценок пока нет
- NCP Impaired Skin IntegrityДокумент1 страницаNCP Impaired Skin Integritysinister17Оценок пока нет
- NCP HyperthermiaДокумент3 страницыNCP HyperthermiaMarla NavarroОценок пока нет
- NCP DengueДокумент3 страницыNCP DenguejhaninahОценок пока нет
- College of Health Sciences: Urdaneta City UniversityДокумент7 страницCollege of Health Sciences: Urdaneta City UniversityDan Dan ManaoisОценок пока нет
- DENGUE CS NCP 1Документ8 страницDENGUE CS NCP 1Karyl SaavedraОценок пока нет
- NCP3 Skin IntegrityДокумент3 страницыNCP3 Skin IntegritySheng Arquiza67% (3)
- Pathophysiology of PTB (Myrc)Документ2 страницыPathophysiology of PTB (Myrc)Rj MagpayoОценок пока нет
- NCP For PCAPCДокумент6 страницNCP For PCAPCEnrique Lu100% (1)
- NCP For Risk of Infectiong R/T Indwelling Catheter Post PartumДокумент1 страницаNCP For Risk of Infectiong R/T Indwelling Catheter Post PartumJared Mabulay100% (1)
- Nursing Care PlansДокумент14 страницNursing Care PlansTels Dela PeñaОценок пока нет
- NCP For EclampsiaДокумент6 страницNCP For EclampsiaXtine Soliman Zamora100% (3)
- NCP TahbsoДокумент18 страницNCP TahbsoKe EjieОценок пока нет
- 5 Benign Febrile Convulsions Nursing Care PlansДокумент19 страниц5 Benign Febrile Convulsions Nursing Care PlansRoanna Alyssa Sy Jimenez75% (4)
- NCP DMДокумент21 страницаNCP DMKate ManalastasОценок пока нет
- Cues Nursing Diagnosis Analysis Planning Intervention Rationale EvaluationДокумент2 страницыCues Nursing Diagnosis Analysis Planning Intervention Rationale EvaluationMark Jaco AngОценок пока нет
- NCPДокумент14 страницNCPclaidelynОценок пока нет
- Management of Dengue Hemorrhagic FeverДокумент7 страницManagement of Dengue Hemorrhagic FeverjoycevillamorОценок пока нет
- NCP Ineffective Tissue Perfusion and Self Care DeficitДокумент5 страницNCP Ineffective Tissue Perfusion and Self Care DeficitFrances Anne Pasiliao100% (3)
- Neonatal Sepsis NCPДокумент9 страницNeonatal Sepsis NCPHollan Galicia100% (1)
- Breast CancerДокумент11 страницBreast CancerKier Jucar de GuzmanОценок пока нет
- HospiceДокумент18 страницHospiceLouie James Velasco OstreaОценок пока нет
- Acute GlomerulonephritisДокумент1 страницаAcute GlomerulonephritisKier Jucar de GuzmanОценок пока нет
- 50 Ways To Conserve EnergyДокумент7 страниц50 Ways To Conserve EnergyKier Jucar de GuzmanОценок пока нет
- Drug Study Er2Документ3 страницыDrug Study Er2Kier Jucar de GuzmanОценок пока нет
- Basic Principles of Normal ECG: Prepared By: Ben Ryan Jucay SauceДокумент25 страницBasic Principles of Normal ECG: Prepared By: Ben Ryan Jucay SauceSoySauceОценок пока нет
- Rectal ProlapseДокумент9 страницRectal ProlapseAnjani Putri RetnaninggalihОценок пока нет
- Medical Surgical Nursing ReviewДокумент97 страницMedical Surgical Nursing ReviewBernadeth Josefa BorelaОценок пока нет
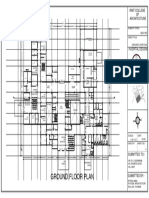
- Ground Floor Plan Sheet 2Документ1 страницаGround Floor Plan Sheet 2riteshОценок пока нет
- Radiology Procedure ManualДокумент29 страницRadiology Procedure ManualAnonymous ic2CDkF100% (1)
- PERIMETRY Introduction GuideДокумент70 страницPERIMETRY Introduction GuideDana Andreea Popescu100% (1)
- Nursing Management HydrocephalusДокумент4 страницыNursing Management HydrocephalusPrecious Mae Benologa100% (1)
- GEHC Site Planning Specifications Safety and Specifications PDFДокумент57 страницGEHC Site Planning Specifications Safety and Specifications PDFD&KОценок пока нет
- 11th Grade Before Band Aids TextДокумент1 страница11th Grade Before Band Aids Textعبدالرحمن باجسيرОценок пока нет
- 5 Meo DMTДокумент18 страниц5 Meo DMTJimmy Contreras Rey100% (1)
- Moraxella SPP, Sphingomonas SPPДокумент31 страницаMoraxella SPP, Sphingomonas SPPDayledaniel SorvetoОценок пока нет
- Natrum Group of RemediesДокумент54 страницыNatrum Group of RemediesDaya NidhiОценок пока нет
- The Letter of Intent To Enter PracticeДокумент4 страницыThe Letter of Intent To Enter Practicekazniels100% (1)
- Connecticut Health PlanДокумент2 страницыConnecticut Health PlanHelen BennettОценок пока нет
- PhilHealth Circular No. 14 S. 2018 - CF4Документ3 страницыPhilHealth Circular No. 14 S. 2018 - CF4Toche Doce100% (1)
- Diagnosis and Management of Subarachnoid HemorrhageДокумент25 страницDiagnosis and Management of Subarachnoid HemorrhageMisael ClintonОценок пока нет
- Materi IAI Palangka Raya - Rev PDFДокумент55 страницMateri IAI Palangka Raya - Rev PDFNopernas CahayaОценок пока нет
- Visual NeglectДокумент2 страницыVisual NeglectPierre A. RodulfoОценок пока нет
- Gpat 2019Документ51 страницаGpat 2019Nishabh KushwahaОценок пока нет
- Sodium Chloride (Rock Salt) MSDS: Section 1: Chemical Product and Company IdentificationДокумент6 страницSodium Chloride (Rock Salt) MSDS: Section 1: Chemical Product and Company IdentificationMohamed MaghawryОценок пока нет
- NIPPVДокумент35 страницNIPPVAnusha VergheseОценок пока нет
- JCIA Handbook 2020Документ61 страницаJCIA Handbook 2020WAQASОценок пока нет
- Subtotal Gastrectomy For Gastric CancerДокумент15 страницSubtotal Gastrectomy For Gastric CancerRUBEN DARIO AGRESOTTОценок пока нет
- Duty Report RIWДокумент41 страницаDuty Report RIWRiyan W. PratamaОценок пока нет
- Drug Card BenadrylДокумент1 страницаDrug Card BenadrylAdrianne Bazo100% (1)
- +bashkir State Medical UniversityДокумент2 страницы+bashkir State Medical UniversityCB SharmaОценок пока нет
- Herk Iames Pressley RidgeДокумент3 страницыHerk Iames Pressley Ridgeapi-350759206Оценок пока нет
- Johnson & Johnson Tylenol CrisisДокумент21 страницаJohnson & Johnson Tylenol CrisisArnab Chatterjee100% (2)
- Chocolate and The Brain: Neurobiological Impact of Cocoa Flavanols On Cognition and BehaviorДокумент9 страницChocolate and The Brain: Neurobiological Impact of Cocoa Flavanols On Cognition and BehaviorStefan AvramovskiОценок пока нет
- Director, Office of Workers' Compensation Programs, United States Department of Labor v. August Mangifest, 826 F.2d 1318, 3rd Cir. (1987)Документ27 страницDirector, Office of Workers' Compensation Programs, United States Department of Labor v. August Mangifest, 826 F.2d 1318, 3rd Cir. (1987)Scribd Government DocsОценок пока нет