Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Serology and Ultrasound For Diagnosis of Choledocolitiasis 2014Документ5 страницSerology and Ultrasound For Diagnosis of Choledocolitiasis 2014DannyОценок пока нет
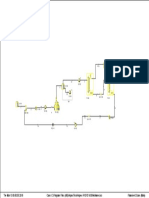
- PFD VCM (Vinyl Chloride Monomer)Документ1 страницаPFD VCM (Vinyl Chloride Monomer)Muhammad Hadi SaputraОценок пока нет
- Cholestasis: Dr. Darmadi SPPD, FinasimДокумент20 страницCholestasis: Dr. Darmadi SPPD, FinasimTiens MonisaОценок пока нет
- Nr. CRT.: Nume, Prenume Varsta (Ani) Sex Sectie de Admisie Foaie de ObservatieДокумент57 страницNr. CRT.: Nume, Prenume Varsta (Ani) Sex Sectie de Admisie Foaie de ObservatieCatalina BuduleciОценок пока нет
- Diagnosis &treatment of Hep CДокумент18 страницDiagnosis &treatment of Hep CMushtaq AhmadОценок пока нет
- Insignis Surgery 2 Gallbladder and Extrahepatic Biliary SystemДокумент7 страницInsignis Surgery 2 Gallbladder and Extrahepatic Biliary SystemPARADISE JanoОценок пока нет
- BilirubinДокумент3 страницыBilirubinIkhza LastPandawaОценок пока нет
- Surgery JournalДокумент23 страницыSurgery JournalRazeen RiyasatОценок пока нет
- Dapus OslerДокумент4 страницыDapus OslerSetyawan Aditya Pambudi SОценок пока нет
- Hepatitis C Treatment Outcome-Dr - MythizheeДокумент28 страницHepatitis C Treatment Outcome-Dr - MythizheevanithaОценок пока нет
- CholecystectomyДокумент6 страницCholecystectomyTom Bayubs-tucsОценок пока нет
- The Accuracy of Fibroscan in A Real World StudyДокумент2 страницыThe Accuracy of Fibroscan in A Real World StudyRaeni Dwi PutriОценок пока нет
- Hepatocellular Carcinoma: Rahela Šafarić, 4th Year 2021/2022Документ15 страницHepatocellular Carcinoma: Rahela Šafarić, 4th Year 2021/2022Rahela WaleОценок пока нет
- Liver Function Reviewer Cc2Документ7 страницLiver Function Reviewer Cc2Leo NoquilОценок пока нет
- Pemeriksaan Fungsi Hati .: Prof. Dr. Adi Koesoema Aman SPPK (KH)Документ51 страницаPemeriksaan Fungsi Hati .: Prof. Dr. Adi Koesoema Aman SPPK (KH)kiki rawitriОценок пока нет
- Feses IntroductionДокумент88 страницFeses IntroductionAnisaPratiwiArumningsih100% (1)
- 34-Paracetamol PoisoningДокумент26 страниц34-Paracetamol PoisoningSumaiyyaОценок пока нет
- Chapter X: Liver Function TestsДокумент20 страницChapter X: Liver Function TestsSasi KumarОценок пока нет
- Pathophysiology - CholedocholithiasisДокумент1 страницаPathophysiology - CholedocholithiasisMark OrculloОценок пока нет
- Gallstone Disease and Acute Cholecystitis MADДокумент21 страницаGallstone Disease and Acute Cholecystitis MADMuhammad AbdurrahmanОценок пока нет
- Overview of HepatopathologyДокумент158 страницOverview of Hepatopathologyamy100% (1)
- Advances in Pathogenesis and Therapeutics of Hepatobiliary DiseasesДокумент192 страницыAdvances in Pathogenesis and Therapeutics of Hepatobiliary DiseasesMiguel SilvaОценок пока нет
- Liver Disease in Pregnancy: DR Amita Suneja Professor, OB & GYN Ucms & GTBHДокумент22 страницыLiver Disease in Pregnancy: DR Amita Suneja Professor, OB & GYN Ucms & GTBHFadil HidayatОценок пока нет
- Hepatitis in Children (Hep A, B, C)Документ26 страницHepatitis in Children (Hep A, B, C)sarОценок пока нет
- Gastroenterology-Liver, Pancreas and Gall Bladder LecturesДокумент7 страницGastroenterology-Liver, Pancreas and Gall Bladder LecturesMarco Paulo Reyes NaoeОценок пока нет
- PSCPBC Infographic v8Документ2 страницыPSCPBC Infographic v8PGold Goodboy Golden RupОценок пока нет
- Liver, Biliary Tree and Pancreas Pathology Lecture Final by DRДокумент94 страницыLiver, Biliary Tree and Pancreas Pathology Lecture Final by DRapi-3700579100% (5)
- Cat Aliza Mehbin BioДокумент1 страницаCat Aliza Mehbin BioKirti DoshiОценок пока нет
- RUQ MassДокумент20 страницRUQ MassCathy CepedaОценок пока нет
- Cholangiocarcinoma, Gallbladder Cancer, Common Bile Duct, Cystic Duct, Intrahepatic, PerihilarДокумент25 страницCholangiocarcinoma, Gallbladder Cancer, Common Bile Duct, Cystic Duct, Intrahepatic, PerihilarMc Crister Silang100% (1)