Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Food Exchange Lists For Meal PlanningДокумент13 страницFood Exchange Lists For Meal PlanningPatricia Young63% (24)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Concept Map of DMДокумент2 страницыConcept Map of DMLeslie Marie Rendon100% (9)
- Ob SkedДокумент1 страницаOb SkedPatricia YoungОценок пока нет
- DM in PregnancyДокумент2 страницыDM in PregnancyPatricia YoungОценок пока нет
- Armynavy Menu 2011Документ1 страницаArmynavy Menu 2011Karen Joyce PinedaОценок пока нет
- Armynavy Menu 2011Документ1 страницаArmynavy Menu 2011Karen Joyce PinedaОценок пока нет
- Armynavy Menu 2011Документ1 страницаArmynavy Menu 2011Karen Joyce PinedaОценок пока нет
- Bullous ImpetigoДокумент6 страницBullous ImpetigoPatricia YoungОценок пока нет
- Cases For DiscussionДокумент2 страницыCases For DiscussionPatricia YoungОценок пока нет
- Blood Sugar 455 MG - DL (25.25mmol - L) and What It Means - BloodSugarEasy PDFДокумент4 страницыBlood Sugar 455 MG - DL (25.25mmol - L) and What It Means - BloodSugarEasy PDFSalman KhanОценок пока нет
- Daftar PustakaДокумент8 страницDaftar PustakaErmaffОценок пока нет
- Nutra Puding Buah NagaДокумент2 страницыNutra Puding Buah NagaUun RochmawatiОценок пока нет
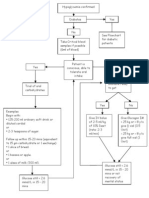
- Hypoglycaemia FlowchartДокумент1 страницаHypoglycaemia FlowchartMohammad SultanОценок пока нет
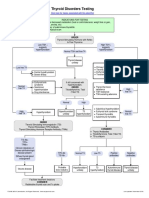
- Thyroid Disorders Testing AlgorithmДокумент1 страницаThyroid Disorders Testing AlgorithmkatОценок пока нет
- Survey of Knowledge-Attitude-Practice (KAP) Concerning Insulin Use in Adult Diabetic Patients at A Tertiary Care HospitalДокумент5 страницSurvey of Knowledge-Attitude-Practice (KAP) Concerning Insulin Use in Adult Diabetic Patients at A Tertiary Care HospitalChandresh DumatarОценок пока нет
- Clew: A37 Cg4+ & G3+ D: I-Stat® Tricontrols Level 1 ControlДокумент4 страницыClew: A37 Cg4+ & G3+ D: I-Stat® Tricontrols Level 1 ControlDominic Isaac AcelajadoОценок пока нет
- Oral Hypoglycemic Drugs2Документ4 страницыOral Hypoglycemic Drugs2علي الطياريОценок пока нет
- THYROID YunitaДокумент81 страницаTHYROID YunitaPandu KusumawardhanyОценок пока нет
- Gliclazide MR, An Efficacy and Safety: For T2DM Patients During RamadanДокумент28 страницGliclazide MR, An Efficacy and Safety: For T2DM Patients During RamadanLeonora KomboyОценок пока нет
- Endocrine Glands PathologyДокумент8 страницEndocrine Glands Pathologychrisp7Оценок пока нет
- Insulin Case Studies AACE 5-20-05Документ56 страницInsulin Case Studies AACE 5-20-05Leanne Shepherd100% (2)
- Thyroid Disorders Testing AlgorithmДокумент1 страницаThyroid Disorders Testing AlgorithmRezi HelperОценок пока нет
- List of Endocrine DiseasesДокумент6 страницList of Endocrine DiseasesPreethiHonavarОценок пока нет
- Gestational DiabetiesДокумент50 страницGestational DiabetiesAkshat Goel100% (1)
- Practical Clinical Endocrinology 2021Документ523 страницыPractical Clinical Endocrinology 2021Morozovschi VitalieОценок пока нет
- Goiter: What Is The Thyroid Gland?Документ2 страницыGoiter: What Is The Thyroid Gland?Julio LeviОценок пока нет
- Garber 2007Документ6 страницGarber 2007Diana SamuezaОценок пока нет
- Thyroid Function TestДокумент31 страницаThyroid Function TestMeno AliОценок пока нет
- Gestational Diabetes Mellitus: Definition, Aetiological and Clinical AspectsДокумент9 страницGestational Diabetes Mellitus: Definition, Aetiological and Clinical AspectsantonellamartОценок пока нет
- Endocrine Pathology LectureДокумент31 страницаEndocrine Pathology Lectureninja2007Оценок пока нет
- Dexamethasone Suppression TestДокумент2 страницыDexamethasone Suppression Testjbeans92Оценок пока нет
- 592008000011: 59000720 03-Aug-20 08:49 AM: Mrs. Veena K Arora: 03-Aug-2020 08:49 AM: Dr. Self: 03-Aug-2020 12:47PM: 48 Y 06 M 12 D / F: 03-Aug-2020 01:12PMДокумент2 страницы592008000011: 59000720 03-Aug-20 08:49 AM: Mrs. Veena K Arora: 03-Aug-2020 08:49 AM: Dr. Self: 03-Aug-2020 12:47PM: 48 Y 06 M 12 D / F: 03-Aug-2020 01:12PMrajanarora72Оценок пока нет
- Discuss Di Erence Between Diabetes Mellitus Type 1 and DM Type 2Документ3 страницыDiscuss Di Erence Between Diabetes Mellitus Type 1 and DM Type 2DHANNILLIE JHAIRA NU�EZОценок пока нет
- A1C InfographicДокумент1 страницаA1C Infographiclewisch81Оценок пока нет
- Endocrine Disorders Julie Mann, NP - Case StudyДокумент10 страницEndocrine Disorders Julie Mann, NP - Case Studysimonedarling75% (4)
- THYROID Nodules PPT June 2013Документ56 страницTHYROID Nodules PPT June 2013GaryОценок пока нет
- GoiterДокумент17 страницGoiterShaimaa EmadОценок пока нет
- Endemic and Sporadic GoiterДокумент13 страницEndemic and Sporadic GoiterBtwo SoelОценок пока нет