Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Consumer Health EducationДокумент21 страницаConsumer Health Educationerwin espinosaОценок пока нет
- Physiotherapy Practices For Patients Undergoing Coronary Artery Bypass Grafting A Cross - Sectional StudyДокумент11 страницPhysiotherapy Practices For Patients Undergoing Coronary Artery Bypass Grafting A Cross - Sectional StudyhayaОценок пока нет
- BASCOLO Et Al - Types of Health Systems Reforms in LA - 2018 PDFДокумент9 страницBASCOLO Et Al - Types of Health Systems Reforms in LA - 2018 PDFJuan ArroyoОценок пока нет
- Laboratory Activity - HIS Lab - iHOMISДокумент2 страницыLaboratory Activity - HIS Lab - iHOMISFrance Cedrick RamosОценок пока нет
- Uterine Fibroids: Frequently Asked Questions FAQ074 Gynecologic ProblemsДокумент3 страницыUterine Fibroids: Frequently Asked Questions FAQ074 Gynecologic ProblemsrohitОценок пока нет
- Module 6Документ22 страницыModule 6Jhoanna Lovely OntulanОценок пока нет
- CBAHI PresentationДокумент23 страницыCBAHI PresentationPrince Jhessie L. AbellaОценок пока нет
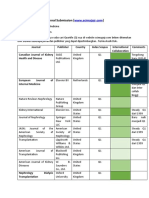
- Journal SubmissionДокумент3 страницыJournal SubmissionMaruhum Bonar MarbunОценок пока нет
- Indian Journal of Applied Basic Medical Science Sept - 2008Документ28 страницIndian Journal of Applied Basic Medical Science Sept - 2008soham2007Оценок пока нет
- Abbott Alinity S FactSheetДокумент1 страницаAbbott Alinity S FactSheetInayat UllahОценок пока нет
- Breast Care in BreastfeedingДокумент11 страницBreast Care in BreastfeedingBella Cy LopezОценок пока нет
- Doctor of Veterinary Medicine: 1st Year 1st SemesterДокумент4 страницыDoctor of Veterinary Medicine: 1st Year 1st SemesterDexter LagrimasОценок пока нет
- International Profiles of Health Care Systems Dec2020Документ228 страницInternational Profiles of Health Care Systems Dec2020GODWIN MAYSON LIWANAGОценок пока нет
- Risk Assessment (Hirarc)Документ17 страницRisk Assessment (Hirarc)MNashОценок пока нет
- Hypotension: Causes, Incidence, and Risk FactorsДокумент4 страницыHypotension: Causes, Incidence, and Risk Factorsclubsanatate100% (1)
- Uterine AtonyДокумент9 страницUterine AtonyElaize Pon Castillo100% (2)
- Case Study Preterm LaborДокумент6 страницCase Study Preterm LaborAdriane ComaОценок пока нет
- PubLSIS II Survey Finding Report June 2018Документ620 страницPubLSIS II Survey Finding Report June 2018Mao udangОценок пока нет
- Epidemiology and Comorbidity of Headache: ReviewДокумент8 страницEpidemiology and Comorbidity of Headache: ReviewConny NapitupuluОценок пока нет
- A Concise Guide To Endodontic Procedures (9783662437292)Документ198 страницA Concise Guide To Endodontic Procedures (9783662437292)ava parham100% (2)
- Daftar PustakaДокумент6 страницDaftar Pustakayazika rimbawatiОценок пока нет
- Stress Testing of Drug SubstancesДокумент29 страницStress Testing of Drug SubstancesMr. HIMANSHU PALIWALОценок пока нет
- Pa Tho Physiology of Hodgkin'sДокумент10 страницPa Tho Physiology of Hodgkin'sIvica Rae100% (1)
- Quintus SlidesCarnivalДокумент103 страницыQuintus SlidesCarnivalmiles sbОценок пока нет
- 5 Minute Veterinary Consult Canine and FelineДокумент1 016 страниц5 Minute Veterinary Consult Canine and FelineMallory Bernstein100% (16)
- Abdominal PainДокумент39 страницAbdominal PainIsma Resti PratiwiОценок пока нет
- A Case of Pleural Effusion With Cardiomegaly Cured With HomoeopathyДокумент9 страницA Case of Pleural Effusion With Cardiomegaly Cured With HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- 102 Written QuestionsДокумент19 страниц102 Written Questionstohomas100% (1)
- Parenteral Nutrition (20 Items)Документ11 страницParenteral Nutrition (20 Items)Ik-ik MiralОценок пока нет
- Recent Advancement in Infertility ManagementДокумент18 страницRecent Advancement in Infertility ManagementFarheen khan100% (2)