Вам также может понравиться
- Humanity's Footprint: Momentum, Impact, and Our Global EnvironmentОт EverandHumanity's Footprint: Momentum, Impact, and Our Global EnvironmentОценок пока нет
- 1990 Health Responsibility Ivan IllichДокумент8 страниц1990 Health Responsibility Ivan IllichclubofcosОценок пока нет
- Mulla Sadra Theory of KnowledgeДокумент29 страницMulla Sadra Theory of Knowledgewww.alhassanain.org.englishОценок пока нет
- The Theory of The Leisure Class - Thorstein VeblenДокумент5 страницThe Theory of The Leisure Class - Thorstein Veblencalukiwa100% (1)
- Guifeng Zongmi-Inquiry Into The Origin of HumanityДокумент20 страницGuifeng Zongmi-Inquiry Into The Origin of HumanityKlaus Fischer100% (1)
- Islam and God-Centricity: Reassessing Fundamental Theological AssumptionsОт EverandIslam and God-Centricity: Reassessing Fundamental Theological AssumptionsОценок пока нет
- M. Fethullah Gulen - The Essentials of The Islamic FaithДокумент223 страницыM. Fethullah Gulen - The Essentials of The Islamic FaithTstre0% (1)
- Psychology, Eschatology, and Imagination in Mulla Sadra's Commentary On Hadith of AwakeningДокумент11 страницPsychology, Eschatology, and Imagination in Mulla Sadra's Commentary On Hadith of AwakeningHaseeb AhmadОценок пока нет
- Beheshti - Philosophy of IslamДокумент335 страницBeheshti - Philosophy of IslamIlmprocessОценок пока нет
- Ibn Al-Arabi and Joseph Campbell Akbari PDFДокумент16 страницIbn Al-Arabi and Joseph Campbell Akbari PDFS⸫Ḥ⸫RОценок пока нет
- Tolerance in BuddhismДокумент11 страницTolerance in Buddhismdaluan2100% (1)
- Sophia - Journal of Traditional Studies - Winter 2007 IssueДокумент70 страницSophia - Journal of Traditional Studies - Winter 2007 IssueDistilledMacrocosm100% (5)
- Structure of Reality in Izutsu's Oriental PhiloДокумент17 страницStructure of Reality in Izutsu's Oriental Philoabouahmad100% (1)
- Einstein God Does Not Play Dice SecДокумент11 страницEinstein God Does Not Play Dice SecyatusacomosaОценок пока нет
- Chittick On JamiДокумент24 страницыChittick On JamiashfaqamarОценок пока нет
- Al Khalq Ayal AllahДокумент55 страницAl Khalq Ayal AllahIslamiaОценок пока нет
- A Glance at Agriculture (Lord Northbourne) PDFДокумент12 страницA Glance at Agriculture (Lord Northbourne) PDFIsraelОценок пока нет
- Andani CrucifixionДокумент20 страницAndani CrucifixionAires Ferreira100% (1)
- Veiled Islam A Deconstructive Sufi FormationДокумент303 страницыVeiled Islam A Deconstructive Sufi FormationMansoor AhmadОценок пока нет
- Understanding Fiqh of MuslimДокумент5 страницUnderstanding Fiqh of MuslimchoronzoneОценок пока нет
- Reason As Balance: The Evolution of AqlДокумент14 страницReason As Balance: The Evolution of Aqljoebob19Оценок пока нет
- Salafism's Historical Framework and the Emergence of Its Creed, Ideology and MethodologyДокумент39 страницSalafism's Historical Framework and the Emergence of Its Creed, Ideology and MethodologyJessica YeoОценок пока нет
- Shunyamurti's journey of self-realizationДокумент7 страницShunyamurti's journey of self-realizationVelinka VekiОценок пока нет
- How Do You Attain The Treasures of Fajr PrayerДокумент4 страницыHow Do You Attain The Treasures of Fajr Prayermarmar92Оценок пока нет
- Jonesn@ceu - Edu: Islamic Feminism in Historical Perspective (2 Credits)Документ14 страницJonesn@ceu - Edu: Islamic Feminism in Historical Perspective (2 Credits)muhammad shibiliОценок пока нет
- Universal Science An Introduction To Islamic MetaphysicsДокумент216 страницUniversal Science An Introduction To Islamic Metaphysicss.ehsan hoseiniОценок пока нет
- An Introduction To Bediuzzaman Said Nursi and The Risale-I Nur CollectionДокумент3 страницыAn Introduction To Bediuzzaman Said Nursi and The Risale-I Nur CollectionShakoorAlamОценок пока нет
- True & False KnowledgeДокумент5 страницTrue & False KnowledgeSakiraОценок пока нет
- William C. Chittick Imaginal Worlds Ibn Al Arabi and The Problem of Religious DiversityДокумент280 страницWilliam C. Chittick Imaginal Worlds Ibn Al Arabi and The Problem of Religious DiversityAhmetОценок пока нет
- Women's Right to Marry Without Guardian Permission in Islamic LawДокумент8 страницWomen's Right to Marry Without Guardian Permission in Islamic LawM Zain Ul AbedinОценок пока нет
- Book Reviews explore religious pluralism and Buddhist teachings on sufferingДокумент3 страницыBook Reviews explore religious pluralism and Buddhist teachings on sufferingashfaqamarОценок пока нет
- The Elements of Islamic Metaphysics - ReviewДокумент3 страницыThe Elements of Islamic Metaphysics - ReviewEdelAliОценок пока нет
- Rizvi - Sabzavari PDFДокумент25 страницRizvi - Sabzavari PDFcoldplaylionОценок пока нет
- Eric Gans - ORIGINARY THINKING - Elements of Generative Anthropology-Stanford University Press (1993)Документ248 страницEric Gans - ORIGINARY THINKING - Elements of Generative Anthropology-Stanford University Press (1993)Cidadaun AnônimoОценок пока нет
- Abdelkader-Modernity, Maslaha and Maqasid in Muslim Legal Thought-Icmr-2003-14-2 PDFДокумент13 страницAbdelkader-Modernity, Maslaha and Maqasid in Muslim Legal Thought-Icmr-2003-14-2 PDFBenett MomoryОценок пока нет
- Janis & Feshback (1953)Документ15 страницJanis & Feshback (1953)Stephanie LynchОценок пока нет
- Only ONE Earth: by Barbara WardДокумент1 страницаOnly ONE Earth: by Barbara WardKoh AhongОценок пока нет
- Being Muslim in The Age of Facebook, Youtube and TwitterДокумент10 страницBeing Muslim in The Age of Facebook, Youtube and TwitterFowad Ahmad100% (1)
- Mulla Sadra's Idea of Existence N Motion in Substance N Its Educational Implications - JavidiДокумент15 страницMulla Sadra's Idea of Existence N Motion in Substance N Its Educational Implications - JavidiSyayhan JindanОценок пока нет
- Yoga Practice Through Merleau-Ponty's Phenomenology of The BodyДокумент11 страницYoga Practice Through Merleau-Ponty's Phenomenology of The BodyIrena Antonijevic100% (1)
- Two Dreams of America - Jacob NeedlemanДокумент42 страницыTwo Dreams of America - Jacob NeedlemanCocceiusОценок пока нет
- Jqs 2018 0315Документ4 страницыJqs 2018 0315Aisyah DamayantiОценок пока нет
- The Paradox of FreedomДокумент18 страницThe Paradox of FreedomPark Sun HaОценок пока нет
- The Ontology of Time in Mulla Sadra's MetaphysicsДокумент1 страницаThe Ontology of Time in Mulla Sadra's MetaphysicsSempiternalОценок пока нет
- Eye of The Heart Issue2 2008Документ138 страницEye of The Heart Issue2 2008gfvilaОценок пока нет
- Al-Mizan (Al I Imran)Документ623 страницыAl-Mizan (Al I Imran)jaamdoctor100% (1)
- William James - The Will To Believe. Human Immortality and Other Essays in Popular Philosophy ##########Документ426 страницWilliam James - The Will To Believe. Human Immortality and Other Essays in Popular Philosophy ##########VandrefalkОценок пока нет
- Revelation, Rationality and Eternal KnowledgeДокумент11 страницRevelation, Rationality and Eternal KnowledgeIbrahim Mahmud MomohОценок пока нет
- (Culture and Civilization in The Middle East 24) Damian A. Howard - Being Human in Islam - The Impact of The Evolutionary Worldview-Routledge (2014)Документ241 страница(Culture and Civilization in The Middle East 24) Damian A. Howard - Being Human in Islam - The Impact of The Evolutionary Worldview-Routledge (2014)Andrés CamposОценок пока нет
- Avicenna'S Eastern ("Oriental") Philosophy Nature, Contents, TransmissionДокумент22 страницыAvicenna'S Eastern ("Oriental") Philosophy Nature, Contents, TransmissionKhouloud AdouliОценок пока нет
- Book of Tawhid Prefacech1Документ26 страницBook of Tawhid Prefacech1YusufAliBahrОценок пока нет
- Jamaat Ul Muslimeen ExposedДокумент36 страницJamaat Ul Muslimeen Exposedsyedshoeb0% (1)
- (Adi Setia) Islamic Ethics in Engagement With Life, Health and MedicineДокумент41 страница(Adi Setia) Islamic Ethics in Engagement With Life, Health and MedicineHajar Almahdaly100% (1)
- Ibrahim Kalin - From Temporal Time To Eternal NowДокумент30 страницIbrahim Kalin - From Temporal Time To Eternal NowAcademixОценок пока нет
- Professor Abdelwhab Elmessiri - Philosophers of The ArabsДокумент43 страницыProfessor Abdelwhab Elmessiri - Philosophers of The Arabssamirabuzaid100% (2)
- Analgesia For Labor and Vaginal DeliveryДокумент21 страницаAnalgesia For Labor and Vaginal DeliveryLouije MombzОценок пока нет
- A Uri Culo TherapyДокумент322 страницыA Uri Culo Therapyserafim67100% (1)
- Transcutaneous Nerve StimulationДокумент6 страницTranscutaneous Nerve StimulationARGОценок пока нет
- Rotator Cuff Assessment PDFДокумент11 страницRotator Cuff Assessment PDFMichele MarengoОценок пока нет
- Unblock Your Abundance by Christie Marie Sheldon Masterclass WorkbookДокумент21 страницаUnblock Your Abundance by Christie Marie Sheldon Masterclass WorkbookMarta Morales KlingeОценок пока нет
- Difficult Patient Encounters: Assessing Pediatric Residents' Communication Skills Training NeedsДокумент19 страницDifficult Patient Encounters: Assessing Pediatric Residents' Communication Skills Training NeedsJesse M. MassieОценок пока нет
- 600 Confusing English Words ExplainedДокумент209 страниц600 Confusing English Words Explainedata nazariОценок пока нет
- Wa0001Документ1 страницаWa0001Boru RajaОценок пока нет
- Focus On Diagnosis of Acute Compartment Syndrome PDFДокумент8 страницFocus On Diagnosis of Acute Compartment Syndrome PDFMuthia DewiОценок пока нет
- Trigeminal NeuralgiaДокумент6 страницTrigeminal NeuralgiaGowriОценок пока нет
- Archons - Your Mind Is Not Your Own...Документ13 страницArchons - Your Mind Is Not Your Own...us4loveОценок пока нет
- Neck Disability IndexДокумент1 страницаNeck Disability IndexPowChoyОценок пока нет
- NURSING CARE PLAN FOR ACUTE PAIN MANAGEMENTДокумент2 страницыNURSING CARE PLAN FOR ACUTE PAIN MANAGEMENTRachel TiangcoОценок пока нет
- Critical thinking exercises for therapeutic communicationДокумент2 страницыCritical thinking exercises for therapeutic communicationLuisz PalmaОценок пока нет
- Chapter 8. Pain Pathways and Mechanisms of The Pulpodentin Complex - CompressedДокумент26 страницChapter 8. Pain Pathways and Mechanisms of The Pulpodentin Complex - CompressedPaola cruzОценок пока нет
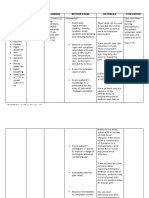
- Assessment Diagnosis Planning Intervention Rationale EvaluationДокумент5 страницAssessment Diagnosis Planning Intervention Rationale EvaluationArian May MarcosОценок пока нет
- The Effect of The Facilitated Tucking Position in Reducing Vaccination-Induced Pain in NewbornsДокумент7 страницThe Effect of The Facilitated Tucking Position in Reducing Vaccination-Induced Pain in NewbornsCassanovaNovaОценок пока нет
- Dark Chocolate's Health BenefitsДокумент13 страницDark Chocolate's Health BenefitsGec Anthony CubillanОценок пока нет
- A Snapshot of Demand For Adult-Use Cannabis in IllinoisДокумент27 страницA Snapshot of Demand For Adult-Use Cannabis in IllinoisTodd FeurerОценок пока нет
- Management of Musculoskeletal DisordersДокумент69 страницManagement of Musculoskeletal DisordersJSeasharkОценок пока нет
- Slide Jurnal Reading 2Документ20 страницSlide Jurnal Reading 2WulanSyafitriОценок пока нет
- Corporal PunishmentДокумент4 страницыCorporal Punishmentabdulhadi masoodОценок пока нет
- Led Light Therapy GuideДокумент23 страницыLed Light Therapy GuidePeter Freimann100% (4)
- Egyptian Healing RODSДокумент67 страницEgyptian Healing RODSŽarko Dačević100% (8)
- Nama: Rohmayati Kelas: 5 I Keperawatan: Yes, She WasДокумент3 страницыNama: Rohmayati Kelas: 5 I Keperawatan: Yes, She WasBuat Aplod0% (1)
- Acute Pain NCPДокумент2 страницыAcute Pain NCPkrz05Оценок пока нет
- PNLE Reviewer With Rationale 1Документ12 страницPNLE Reviewer With Rationale 1Zyla Malinao100% (1)
- Psychiartry NotesДокумент38 страницPsychiartry NotesAlthea Lujille PinazoОценок пока нет
- Paracervical block technique and complicationsДокумент4 страницыParacervical block technique and complicationspolygoneОценок пока нет
- Assessing The Reliability and Responsiveness of 5 Shoulder QuestionnairesДокумент8 страницAssessing The Reliability and Responsiveness of 5 Shoulder QuestionnairesJanaiana UchoaОценок пока нет
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (13)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 3.5 из 5 звезд3.5/5 (2)
- The Wicked and the Willing: An F/F Gothic Horror Vampire NovelОт EverandThe Wicked and the Willing: An F/F Gothic Horror Vampire NovelРейтинг: 4 из 5 звезд4/5 (21)
- Prisoners of Geography: Ten Maps That Explain Everything About the WorldОт EverandPrisoners of Geography: Ten Maps That Explain Everything About the WorldРейтинг: 4.5 из 5 звезд4.5/5 (1143)
- Selling the Dream: The Billion-Dollar Industry Bankrupting AmericansОт EverandSelling the Dream: The Billion-Dollar Industry Bankrupting AmericansРейтинг: 4 из 5 звезд4/5 (17)
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndОт EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndОценок пока нет
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (44)
- 1177 B.C.: The Year Civilization Collapsed: Revised and UpdatedОт Everand1177 B.C.: The Year Civilization Collapsed: Revised and UpdatedРейтинг: 4.5 из 5 звезд4.5/5 (109)
- Troubled: A Memoir of Foster Care, Family, and Social ClassОт EverandTroubled: A Memoir of Foster Care, Family, and Social ClassРейтинг: 4.5 из 5 звезд4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Dark Psychology: Discover How To Analyze People and Master Human Manipulation Using Body Language Secrets, Covert NLP, Mind Control, Subliminal Persuasion, Hypnosis, and Speed Reading Techniques.От EverandDark Psychology: Discover How To Analyze People and Master Human Manipulation Using Body Language Secrets, Covert NLP, Mind Control, Subliminal Persuasion, Hypnosis, and Speed Reading Techniques.Рейтинг: 4.5 из 5 звезд4.5/5 (88)
- The Exvangelicals: Loving, Living, and Leaving the White Evangelical ChurchОт EverandThe Exvangelicals: Loving, Living, and Leaving the White Evangelical ChurchРейтинг: 4.5 из 5 звезд4.5/5 (12)
- Hey, Hun: Sales, Sisterhood, Supremacy, and the Other Lies Behind Multilevel MarketingОт EverandHey, Hun: Sales, Sisterhood, Supremacy, and the Other Lies Behind Multilevel MarketingРейтинг: 4 из 5 звезд4/5 (102)
- The Body Is Not an Apology, Second Edition: The Power of Radical Self-LoveОт EverandThe Body Is Not an Apology, Second Edition: The Power of Radical Self-LoveРейтинг: 4.5 из 5 звезд4.5/5 (365)
- His Needs, Her Needs: Building a Marriage That LastsОт EverandHis Needs, Her Needs: Building a Marriage That LastsРейтинг: 4.5 из 5 звезд4.5/5 (100)
- Little Princes: One Man's Promise to Bring Home the Lost Children of NepalОт EverandLittle Princes: One Man's Promise to Bring Home the Lost Children of NepalОценок пока нет
- American Jezebel: The Uncommon Life of Anne Hutchinson, the Woman Who Defied the PuritansОт EverandAmerican Jezebel: The Uncommon Life of Anne Hutchinson, the Woman Who Defied the PuritansРейтинг: 3.5 из 5 звезд3.5/5 (66)
- Double Lives: True Tales of the Criminals Next DoorОт EverandDouble Lives: True Tales of the Criminals Next DoorРейтинг: 4 из 5 звезд4/5 (34)
- Perfect Murder, Perfect Town: The Uncensored Story of the JonBenet Murder and the Grand Jury's Search for the TruthОт EverandPerfect Murder, Perfect Town: The Uncensored Story of the JonBenet Murder and the Grand Jury's Search for the TruthРейтинг: 3.5 из 5 звезд3.5/5 (68)
- Crypt: Life, Death and Disease in the Middle Ages and BeyondОт EverandCrypt: Life, Death and Disease in the Middle Ages and BeyondРейтинг: 4 из 5 звезд4/5 (3)
- Be a Revolution: How Everyday People Are Fighting Oppression and Changing the World—and How You Can, TooОт EverandBe a Revolution: How Everyday People Are Fighting Oppression and Changing the World—and How You Can, TooРейтинг: 5 из 5 звезд5/5 (1)