Вам также может понравиться
- Nbme 18Документ49 страницNbme 18Dilawar Jan95% (38)
- PBLДокумент8 страницPBLJellou MacОценок пока нет
- Essentials of Abnormal Psychology 8th Edition Durand Test Bank DownloadДокумент38 страницEssentials of Abnormal Psychology 8th Edition Durand Test Bank DownloadcarrielivingstonocifrtkgnyОценок пока нет
- Cardiac Case Study #2Документ2 страницыCardiac Case Study #2Donna LLerandiОценок пока нет
- Ati QuestionsДокумент2 страницыAti Questionsnjames44Оценок пока нет
- TPNДокумент56 страницTPNdenekeОценок пока нет
- Normocytic Anemia'sДокумент14 страницNormocytic Anemia'sbrown_chocolate87643Оценок пока нет
- Cesarean Section: Yusef C. Wibowo, S.ST.,M.HДокумент6 страницCesarean Section: Yusef C. Wibowo, S.ST.,M.HberlyanaОценок пока нет
- Pregnancy Induced Hypertension (PIH) : Case Scenario 4Документ4 страницыPregnancy Induced Hypertension (PIH) : Case Scenario 4Mae Arra Lecobu-anОценок пока нет
- Protein Calorie MalnutritionДокумент97 страницProtein Calorie Malnutritionnshaikh56Оценок пока нет
- Tube FeedingДокумент47 страницTube FeedingArlyn Mendenilla0% (1)
- Antihyperlipidemic Drugs: Key Terms Chapter ObjectivesДокумент9 страницAntihyperlipidemic Drugs: Key Terms Chapter ObjectivesSasa AbassОценок пока нет
- Carbohydrate - Modified Diets For Malabsorption SyndromesДокумент51 страницаCarbohydrate - Modified Diets For Malabsorption SyndromesJustKath OneseventwoОценок пока нет
- Drugs in ObstetricsДокумент95 страницDrugs in ObstetricsPriya jОценок пока нет
- Nutritional Issues in The ICU Case FileДокумент2 страницыNutritional Issues in The ICU Case Filehttps://medical-phd.blogspot.com100% (1)
- Medicine and Nutrition Case StudyДокумент5 страницMedicine and Nutrition Case Studyapi-384113918Оценок пока нет
- Special DietsДокумент52 страницыSpecial DietsMara Faye R. AvilesОценок пока нет
- Congenital Adrenal HyperplasiaДокумент29 страницCongenital Adrenal HyperplasiaMohan RaoОценок пока нет
- Diabetes Insipidus (Agu Presentation)Документ15 страницDiabetes Insipidus (Agu Presentation)Um HamoOdОценок пока нет
- Diarrhea: ChildrenДокумент16 страницDiarrhea: ChildrenEmmi Valentina PardedeОценок пока нет
- Evaluation of Fetal Well BeingДокумент22 страницыEvaluation of Fetal Well BeingJoanah Mae AsuncionОценок пока нет
- Poisoning in ChildrenДокумент11 страницPoisoning in ChildrenAndriana HalfienОценок пока нет
- First AssessmentДокумент3 страницыFirst AssessmentBianglala OkeОценок пока нет
- Drug Card Solu-MEDROLДокумент2 страницыDrug Card Solu-MEDROLBenОценок пока нет
- Diabetes Mellitus: Dr. Sajid Abbas JaffriДокумент37 страницDiabetes Mellitus: Dr. Sajid Abbas JaffriMaham ZarrinОценок пока нет
- 6-Health Problems Common in PreschoolerДокумент36 страниц6-Health Problems Common in PreschoolerPam Lala100% (2)
- Case StudyДокумент6 страницCase Studyapi-276551783Оценок пока нет
- 1 RicketsДокумент32 страницы1 RicketsDarina Ismakaieva100% (1)
- GSDДокумент26 страницGSDFahad Ali NadeemОценок пока нет
- HypertensionДокумент6 страницHypertensionTj Kevin P-DoctorОценок пока нет
- Hematologic System2Документ70 страницHematologic System2Jesus Mario LopezОценок пока нет
- 1 - Presentation - Management of Preclamplsia, Mild and ModerateДокумент22 страницы1 - Presentation - Management of Preclamplsia, Mild and ModeratesharonОценок пока нет
- Fluid Electrolytes and Acid Base BalanceДокумент108 страницFluid Electrolytes and Acid Base BalancesayednourОценок пока нет
- Hematology & Immune SystemДокумент81 страницаHematology & Immune SystemAmanuel Maru100% (1)
- Hyperprolactinem IaДокумент63 страницыHyperprolactinem Iakhadzx100% (2)
- Pharmacology Exam4 ReviewДокумент8 страницPharmacology Exam4 ReviewNatalia BortellОценок пока нет
- GastroДокумент82 страницыGastroZhailyn Joy DumlaoОценок пока нет
- Epilepsy in Pregnancy JatuДокумент57 страницEpilepsy in Pregnancy Jatuninjahattori1Оценок пока нет
- Concepts of Jaundice by DR SarmaДокумент53 страницыConcepts of Jaundice by DR SarmaAmanuel Maru100% (3)
- Endocrine Med-Surg Slide Show Presentation (Nursing)Документ43 страницыEndocrine Med-Surg Slide Show Presentation (Nursing)loveoverprideОценок пока нет
- Fluid and Electrolyte Therapy - SeblewongelДокумент47 страницFluid and Electrolyte Therapy - SeblewongelSeblewongel AsemeОценок пока нет
- Irritable Bowel SyndromeДокумент22 страницыIrritable Bowel SyndromeMarium NabeelОценок пока нет
- Severe Acute Malnutrition and Fluid Management inДокумент76 страницSevere Acute Malnutrition and Fluid Management inBibsОценок пока нет
- List of Drug OtotoxicДокумент3 страницыList of Drug OtotoxicLukas I Nyoman Yesaya CavinОценок пока нет
- Rle Neonate DrugsДокумент13 страницRle Neonate DrugsLhara Vhaneza CuetoОценок пока нет
- Paediatric Diabetic KetoacidosisДокумент7 страницPaediatric Diabetic KetoacidosisJuan Carlos BayonaОценок пока нет
- Pellagra: Elaborated By:tambur Vadim Group:M2016Документ11 страницPellagra: Elaborated By:tambur Vadim Group:M2016vadim tamburОценок пока нет
- PPP - Kwashiorkor & MarasmusДокумент19 страницPPP - Kwashiorkor & MarasmusJanine Kristine ManaoisОценок пока нет
- Antifungal DrugsДокумент20 страницAntifungal DrugsboeykhОценок пока нет
- Cesarean Section PrimaryДокумент33 страницыCesarean Section PrimaryKazvin Carl PeraltaОценок пока нет
- Renal Disease in PregnancyДокумент28 страницRenal Disease in PregnancysuperjaxxxonОценок пока нет
- Oxytocic & TocolyticДокумент12 страницOxytocic & TocolyticFahmi Dwika Hafiz TrionoОценок пока нет
- DiabeticcasestudyДокумент7 страницDiabeticcasestudyapi-272773859Оценок пока нет
- ShockДокумент21 страницаShockMin-Joo Esther ParkОценок пока нет
- Q Oral Glucose Tolerance TestДокумент4 страницыQ Oral Glucose Tolerance TestNur Amirah FarhanahОценок пока нет
- Asthma (Reactive Airway Disease)Документ33 страницыAsthma (Reactive Airway Disease)anwar jabariОценок пока нет
- Nut116bl Minics 2 Peds Nafld 2017Документ5 страницNut116bl Minics 2 Peds Nafld 2017api-347153077Оценок пока нет
- Chapter 16 Anti InflammДокумент36 страницChapter 16 Anti InflammAngela Joy AmparadoОценок пока нет
- Nsaids 190204194047Документ40 страницNsaids 190204194047Harini Bala100% (1)
- Anti Diabetic DrugsДокумент58 страницAnti Diabetic DrugsDaniel WangОценок пока нет
- Gestational Hypertension-MeДокумент32 страницыGestational Hypertension-Mekurt94764Оценок пока нет
- Plasma ProteinДокумент79 страницPlasma ProteinnadieОценок пока нет
- Fluid and Elctrolyte Balance.... Power PointДокумент40 страницFluid and Elctrolyte Balance.... Power PointMarwan M.100% (1)
- MedicineДокумент48 страницMedicineKasun Perera0% (1)
- Teachers Health Examination FormДокумент2 страницыTeachers Health Examination FormRosemarie Ceredon ChyОценок пока нет
- Prof Dennis Yue Kellion LectureДокумент55 страницProf Dennis Yue Kellion LectureOhoud ElsheikhОценок пока нет
- Neuro QuizДокумент47 страницNeuro QuizMeredith Caitlyn Fernandez100% (1)
- Cronic Heart Failure - EscДокумент55 страницCronic Heart Failure - EscRisti Graharti100% (1)
- Amoxicillin + HydrochlorothiazideДокумент1 страницаAmoxicillin + HydrochlorothiazideAnonymous wmF9p2ejОценок пока нет
- Arihan Gupta Research Assessment 6 3Документ3 страницыArihan Gupta Research Assessment 6 3api-529369011Оценок пока нет
- Terazosin Drug Study Group 4Документ3 страницыTerazosin Drug Study Group 4Michelle Dona MirallesОценок пока нет
- Blood Pressure Measurement in Children andДокумент7 страницBlood Pressure Measurement in Children andHartanto SantosoОценок пока нет
- NewДокумент34 страницыNewAgatha NindaОценок пока нет
- Schweiz-Health - PhytoD3 - 2013 - Kent KomaeДокумент28 страницSchweiz-Health - PhytoD3 - 2013 - Kent KomaeZayn DeruloОценок пока нет
- Early Onset Type 2 Diabetes: Risk Factors, Clinical Impact and ManagementДокумент11 страницEarly Onset Type 2 Diabetes: Risk Factors, Clinical Impact and ManagementMuhammad Hafidzul HairulОценок пока нет
- Teacher Health CardДокумент1 страницаTeacher Health CardMaria Fatima ArnaizОценок пока нет
- Webminar: Hypertension and Diabetes Mellitus Management in Clinical PracticesДокумент37 страницWebminar: Hypertension and Diabetes Mellitus Management in Clinical PracticesSans 88Оценок пока нет
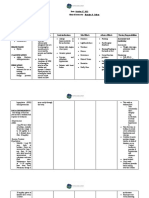
- NCP Preeclampsia and EclampsiaДокумент16 страницNCP Preeclampsia and EclampsiaBiway Regala100% (1)
- HTN Treatment AlgorithmДокумент1 страницаHTN Treatment AlgorithmKati GrissomОценок пока нет
- Value of Participating in Physical ActivitiesДокумент4 страницыValue of Participating in Physical ActivitiesMyko Gorospe33% (3)
- E52 Omron SEM-1 (HEM-7051-C12) ESHДокумент6 страницE52 Omron SEM-1 (HEM-7051-C12) ESHipsrsОценок пока нет
- 3 Series Upper Arm Blood Pressure Monitor: Instruction ManualДокумент30 страниц3 Series Upper Arm Blood Pressure Monitor: Instruction ManualAlОценок пока нет
- NURS FPX 6614 Assessment 1 Defining A Gap in PracticeДокумент6 страницNURS FPX 6614 Assessment 1 Defining A Gap in PracticeCarolyn HarkerОценок пока нет
- Cardiovascular NCLEX QuestionsДокумент12 страницCardiovascular NCLEX QuestionsAivan Karl AmbaganОценок пока нет
- Modular CG NightДокумент5 страницModular CG NightGenie SorianoОценок пока нет
- Renal Cell CancerДокумент575 страницRenal Cell CancerIon VasianОценок пока нет
- Practice 4Документ11 страницPractice 4Justine Rs Dela TorreОценок пока нет
- NCP Discharge PlanningДокумент7 страницNCP Discharge PlanningMarcieОценок пока нет
- BibliographyДокумент2 страницыBibliographyMajkel Benche CustodioОценок пока нет