Вам также может понравиться
- Gender SensitivityДокумент10 страницGender Sensitivityapi-3704562100% (10)
- Gender SensitivityДокумент2 страницыGender Sensitivityapi-370456296% (26)
- PulmoconДокумент64 страницыPulmoconapi-3704562100% (1)
- SURGERYДокумент36 страницSURGERYapi-3704562Оценок пока нет
- Dr. JTG Presentation (Diarrheas)Документ33 страницыDr. JTG Presentation (Diarrheas)api-3704562Оценок пока нет
- Kaplan Community EpidemДокумент3 страницыKaplan Community Epidemapi-3704562Оценок пока нет
- PlasticischwartsДокумент3 страницыPlasticischwartsapi-3704562Оценок пока нет
- Neurosurgery Case 1Документ111 страницNeurosurgery Case 1api-3704562Оценок пока нет
- Vasculitis SyndromesДокумент9 страницVasculitis Syndromesapi-3704562Оценок пока нет
- SLE SummaryДокумент5 страницSLE Summaryapi-3704562100% (1)
- Psych AdjustmentДокумент2 страницыPsych Adjustmentapi-3704562Оценок пока нет
- CHAPTER 127 MENINGOCOCCAL INFECTIONS SummaryДокумент3 страницыCHAPTER 127 MENINGOCOCCAL INFECTIONS Summaryapi-3704562Оценок пока нет
- Bacterial and Viral MeningitisДокумент12 страницBacterial and Viral Meningitisapi-3704562100% (1)
- HUMAN HERPES VIRUS Types 6Документ1 страницаHUMAN HERPES VIRUS Types 6api-3704562100% (1)
- Ringkasan MeningitisДокумент2 страницыRingkasan Meningitisd17oОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- YS 700W Bifacial Solar PanelДокумент2 страницыYS 700W Bifacial Solar PanelDaniel RodriguezОценок пока нет
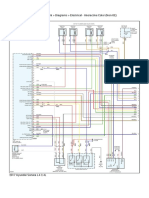
- 2017 Hyundai Sonata L4-2.4L Engine Controls (Powertrain Management) - ALLDATA RepairДокумент6 страниц2017 Hyundai Sonata L4-2.4L Engine Controls (Powertrain Management) - ALLDATA RepairChino PlagaОценок пока нет
- Tycho BraheДокумент3 страницыTycho BraheAienna Lacaya MatabalanОценок пока нет
- BS en 6100-3-2 Electromagnetic Compatibility (EMC)Документ12 страницBS en 6100-3-2 Electromagnetic Compatibility (EMC)Arun Jacob CherianОценок пока нет
- Shri Fa 4Документ44 страницыShri Fa 4Veena H NayakОценок пока нет
- Omnivision Man lp06xx Rev0 0611Документ18 страницOmnivision Man lp06xx Rev0 0611ivan ramirezОценок пока нет
- Maths Class Xii Sample Paper Test 02 For Board Exam 2023Документ6 страницMaths Class Xii Sample Paper Test 02 For Board Exam 2023Priyanshu KasanaОценок пока нет
- Effect of Calorie Restriction and Exercise On Type 2 DiabetesДокумент18 страницEffect of Calorie Restriction and Exercise On Type 2 DiabetesDitya Monica 065Оценок пока нет
- QW PDFДокумент45 страницQW PDFkarthikeyan PОценок пока нет
- LightsДокумент33 страницыLightsEduardo Almeida SilvaОценок пока нет
- Classification of Tooth StainingДокумент4 страницыClassification of Tooth StainingYAMUNA M.D.S. PAEDODONTICS & PREVENTIVE DENTISTRYОценок пока нет
- Furuno FM 8700 Users Manual 429122Документ102 страницыFuruno FM 8700 Users Manual 429122Igor MaranguanheОценок пока нет
- Kyocera 1800Документ2 страницыKyocera 1800gendoetzОценок пока нет
- Module Letter 1Документ2 страницыModule Letter 1eeroleОценок пока нет
- FutbolistaДокумент18 страницFutbolistaKaren Osses50% (2)
- Roadmap: B1+ Students' Book Audio ScriptsДокумент44 страницыRoadmap: B1+ Students' Book Audio ScriptsThanh Dat Phan100% (4)
- Lesson 4Документ10 страницLesson 4Nagiri MuraliОценок пока нет
- Seismic Retrofitting2.0 BY PRIYANSHUДокумент30 страницSeismic Retrofitting2.0 BY PRIYANSHUPriyanshu VarshneyОценок пока нет
- DE (Diatomaceous Earth) BenefitsДокумент9 страницDE (Diatomaceous Earth) BenefitsIlqa116100% (1)
- Morning in Nagrebcan - Manuel E. ArguillaДокумент8 страницMorning in Nagrebcan - Manuel E. ArguillaClara Buenconsejo75% (16)
- 4.dole Regulations On Safety Standards in ConstrДокумент31 страница4.dole Regulations On Safety Standards in Constrmacky02 sorenatsacОценок пока нет
- I10 Workshop Manual - AДокумент292 страницыI10 Workshop Manual - ANorthstartechnology Company82% (11)
- Agriculture Mcqs PDFДокумент4 страницыAgriculture Mcqs PDFAbdul QudoosОценок пока нет
- Civil 416Документ2 страницыCivil 416tskh11Оценок пока нет
- Chapter Eight - Vapour Compression CycleДокумент37 страницChapter Eight - Vapour Compression Cyclealhusseny100% (1)
- Marxist Study of The God of Small ThingsДокумент11 страницMarxist Study of The God of Small ThingsIsrar KhanОценок пока нет
- Nonlinear Analysis and Optimal Design of Reinforced Concrete Plates and ShellsДокумент17 страницNonlinear Analysis and Optimal Design of Reinforced Concrete Plates and Shellsrodain najjarОценок пока нет
- Labangon Elementary School Diagbostic Test in Epp/Tle 6 Directions: Multiple Choice. Choose The Correct The Letter of The Correct AnswerДокумент4 страницыLabangon Elementary School Diagbostic Test in Epp/Tle 6 Directions: Multiple Choice. Choose The Correct The Letter of The Correct AnswerJulianFlorenzFalconeОценок пока нет
- CON21 6th EditionДокумент65 страницCON21 6th EditionDavid WeeОценок пока нет
- X-Ray Radiation and Gamma RadiationДокумент13 страницX-Ray Radiation and Gamma RadiationVence MeraОценок пока нет