Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Blood Coagulation Overview and Inherited Hemorrhagic Disorders Questions 2Документ25 страницBlood Coagulation Overview and Inherited Hemorrhagic Disorders Questions 2John M. Hemsworth50% (2)
- 2021-04-15-Research On Global M-Blood Plasma Products Market in India 2021-91975860Документ64 страницы2021-04-15-Research On Global M-Blood Plasma Products Market in India 2021-91975860Vivek SrinivasanОценок пока нет
- Artis Zee Brochure 28193940 1Документ12 страницArtis Zee Brochure 28193940 1AmritОценок пока нет
- Endovascular Fistula Symposium: 3rd December 2014 (Wednesday)Документ1 страницаEndovascular Fistula Symposium: 3rd December 2014 (Wednesday)AmritОценок пока нет
- Radiographics.21.suppl 1.g01oc11s17Документ19 страницRadiographics.21.suppl 1.g01oc11s17AmritОценок пока нет
- Iv. Guidance Chapter: Bi-Rads - MammographyДокумент7 страницIv. Guidance Chapter: Bi-Rads - MammographyAmritОценок пока нет
- Microwave Ablation of Hepatic MalignancyДокумент11 страницMicrowave Ablation of Hepatic MalignancyAmritОценок пока нет
- Lifecath & Maxflo: Picc CTДокумент12 страницLifecath & Maxflo: Picc CTAmritОценок пока нет
- Thermal Ablation of Tumours: Biological Mechanisms and Advances in TherapyДокумент10 страницThermal Ablation of Tumours: Biological Mechanisms and Advances in TherapyAmritОценок пока нет
- The Birth, Early Years, and Future of Interventional RadiologyДокумент13 страницThe Birth, Early Years, and Future of Interventional RadiologyAmritОценок пока нет
- Breast Interventions: A Primer For Interventional RadiologistsДокумент6 страницBreast Interventions: A Primer For Interventional RadiologistsAmritОценок пока нет
- Update On Preoperative Breast Localization: Radiologic Clinics of North America May 2017Документ14 страницUpdate On Preoperative Breast Localization: Radiologic Clinics of North America May 2017AmritОценок пока нет
- Microwave Ablation of Osteoid OsteomasДокумент2 страницыMicrowave Ablation of Osteoid OsteomasAmritОценок пока нет
- Sclerotherapy With Polidocanol For Treatment of AnДокумент4 страницыSclerotherapy With Polidocanol For Treatment of AnAmritОценок пока нет
- NepalДокумент26 страницNepalkishanadhОценок пока нет
- Sample PDFДокумент10 страницSample PDFkumarank12Оценок пока нет
- Dycaico v. SSSДокумент4 страницыDycaico v. SSSMelissa Mae Cailon MareroОценок пока нет
- Supreme Court Rules Assault Murder Under IPC Section 300Документ13 страницSupreme Court Rules Assault Murder Under IPC Section 300Rajan MeenaОценок пока нет
- PR DR Coana - IntanArdylaMДокумент140 страницPR DR Coana - IntanArdylaMAnnisa Tria FadillaОценок пока нет
- Access To Special Care Dentistry, Part 5. Safety: A. Dougall and J. FiskeДокумент14 страницAccess To Special Care Dentistry, Part 5. Safety: A. Dougall and J. FiskeMostafa FayadОценок пока нет
- Cereno vs. Court of AppealsДокумент2 страницыCereno vs. Court of AppealsAndrea GarciaОценок пока нет
- PDF Eapp 111 Second Quarter Exam - CompressДокумент25 страницPDF Eapp 111 Second Quarter Exam - CompressLilibeth PalangdaoОценок пока нет
- Assessing Risk of Bleeding in a Patient with Acute GastroenteritisДокумент3 страницыAssessing Risk of Bleeding in a Patient with Acute GastroenteritisAce Dioso Tubasco100% (2)
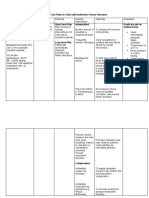
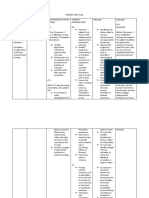
- Nursing Care Plan For Client With Ineffective Tissue PerfusionДокумент2 страницыNursing Care Plan For Client With Ineffective Tissue PerfusionThe Right WayОценок пока нет
- Quiz - Hemodynamic Disorders, Thromboembolic DiseaДокумент48 страницQuiz - Hemodynamic Disorders, Thromboembolic DiseaAdrian CaballesОценок пока нет
- Nursing Care Plan Placenta PreviaДокумент2 страницыNursing Care Plan Placenta Previaderic98% (42)
- Haem. Notes (MBCHB) ProperДокумент162 страницыHaem. Notes (MBCHB) ProperKelvinTMaikanaОценок пока нет
- E Nursing LFDДокумент2 страницыE Nursing LFDAlhadzra AlihОценок пока нет
- AngiofibromaДокумент7 страницAngiofibromaPandu DiputraОценок пока нет
- Complications of Bleeding Disorders in PregnancyДокумент11 страницComplications of Bleeding Disorders in PregnancyNursing ReviewerОценок пока нет
- Legal Med Physical InjuriesДокумент78 страницLegal Med Physical InjuriesTammy YahОценок пока нет
- Stomach and DuodenumДокумент84 страницыStomach and DuodenumDhanush PillaiОценок пока нет
- Nursing Care Plan and FdarДокумент6 страницNursing Care Plan and FdarCheska YsabelleОценок пока нет
- Preoperative HO RanyДокумент35 страницPreoperative HO RanyRMRОценок пока нет
- Hematologic DiseasesДокумент13 страницHematologic DiseaseshithОценок пока нет
- HemophiliaДокумент60 страницHemophiliavibhurocksОценок пока нет
- Hypovolemic Shock Nursing Care Management and Study GuideДокумент1 страницаHypovolemic Shock Nursing Care Management and Study GuideRoselyn VelascoОценок пока нет
- High PlateletsДокумент9 страницHigh PlateletsHemal VyasОценок пока нет
- Nursing Care Plan (NCP) For Acute Lymphocytic LeukemiaДокумент4 страницыNursing Care Plan (NCP) For Acute Lymphocytic LeukemiaromelynОценок пока нет
- Nurse Practitioners, Medical Negligence and Crime: A Case StudyДокумент8 страницNurse Practitioners, Medical Negligence and Crime: A Case StudyJose BernelОценок пока нет
- NCP Format LatestДокумент5 страницNCP Format LatestPrinceОценок пока нет
- Massive Transfusion - StatPearls - NCBI BookshelfДокумент6 страницMassive Transfusion - StatPearls - NCBI Bookshelfsadam sodomОценок пока нет
- Atlas of Operative Maxillofacial Trauma Surgery Primary Repair of Facial Injuries (UnitedVRG)Документ834 страницыAtlas of Operative Maxillofacial Trauma Surgery Primary Repair of Facial Injuries (UnitedVRG)Ahmad YОценок пока нет
- Scarpelli EM, Regional Anesthesia and Anticoagulation, Narrative Review Current Considerations, IAC 2024Документ9 страницScarpelli EM, Regional Anesthesia and Anticoagulation, Narrative Review Current Considerations, IAC 2024jorge fabregatОценок пока нет