Вам также может понравиться
- Course Projects PDFДокумент1 страницаCourse Projects PDFsanjog kshetriОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Manual Samsung Galaxy S Duos GT-S7562Документ151 страницаManual Samsung Galaxy S Duos GT-S7562montesjjОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
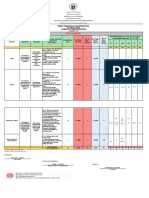
- Revised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10Документ6 страницRevised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10May Ann GuintoОценок пока нет
- Bushcraft Knife AnatomyДокумент2 страницыBushcraft Knife AnatomyCristian BotozisОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Protection in Distributed GenerationДокумент24 страницыProtection in Distributed Generationbal krishna dubeyОценок пока нет
- Sistine Chapel Ceiling Lesson PlanДокумент28 страницSistine Chapel Ceiling Lesson PlannivamОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- ArcGIS Shapefile Files Types & ExtensionsДокумент4 страницыArcGIS Shapefile Files Types & ExtensionsdanangОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- DISCHARGE PLAN CuyosДокумент6 страницDISCHARGE PLAN CuyosShaweeyah Mariano BabaoОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Packet Unit 3 - Atomic Structure-Answers ChemistryДокумент11 страницPacket Unit 3 - Atomic Structure-Answers ChemistryMario J. KafatiОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Unit 1 - Lecture 3Документ16 страницUnit 1 - Lecture 3Abhay kushwahaОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- De DusterДокумент6 страницDe DusterArstОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Docsity Detailed Lesson Plan 5Документ4 страницыDocsity Detailed Lesson Plan 5Sydie MoredoОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- 1 - Laminar and Turbulent Flow - MITWPU - HP - CDK PDFДокумент13 страниц1 - Laminar and Turbulent Flow - MITWPU - HP - CDK PDFAbhishek ChauhanОценок пока нет
- Ideal Gas Law Lesson Plan FinalДокумент5 страницIdeal Gas Law Lesson Plan FinalLonel SisonОценок пока нет
- Fmicb 10 02876Документ11 страницFmicb 10 02876Angeles SuarezОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Invoices For UEG IstanbulДокумент7 страницInvoices For UEG IstanbulIesaw IesawОценок пока нет
- Specification Sheet: Case I Case Ii Operating ConditionsДокумент1 страницаSpecification Sheet: Case I Case Ii Operating ConditionsKailas NimbalkarОценок пока нет
- Centrifuge ThickeningДокумент8 страницCentrifuge ThickeningenviroashОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Brochure International ConferenceДокумент6 страницBrochure International ConferenceAnubhav Sharma sf 12Оценок пока нет
- Information Technology Project Management: by Jack T. MarchewkaДокумент44 страницыInformation Technology Project Management: by Jack T. Marchewkadeeps0705Оценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Discovery and Integration Content Guide - General ReferenceДокумент37 страницDiscovery and Integration Content Guide - General ReferencerhocuttОценок пока нет
- Introduction To M365 PresentationДокумент50 страницIntroduction To M365 Presentationlasidoh0% (1)
- CSEC SocStud CoverSheetForESBA Fillable Dec2019Документ1 страницаCSEC SocStud CoverSheetForESBA Fillable Dec2019chrissaineОценок пока нет
- MV Lec PDFДокумент102 страницыMV Lec PDFJonas Datu100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Restaurant Report Card: February 9, 2023Документ4 страницыRestaurant Report Card: February 9, 2023KBTXОценок пока нет
- 1996 OKI LCD Driver Controller DatabookДокумент232 страницы1996 OKI LCD Driver Controller Databookpiptendo100% (1)
- Uneb U.C.E Mathematics Paper 1 2018Документ4 страницыUneb U.C.E Mathematics Paper 1 2018shafickimera281Оценок пока нет
- Activity Evaluation Form: "Where Children Come First"Документ1 страницаActivity Evaluation Form: "Where Children Come First"TuTitОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Fair & LovelyДокумент10 страницFair & LovelyAymanCheema100% (3)
- Suspend and Resume Calls: Exit PlugДокумент4 страницыSuspend and Resume Calls: Exit PlugrajuОценок пока нет