Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Tracheostomy Suctioning ChildДокумент3 страницыTracheostomy Suctioning ChildKeila RosalesОценок пока нет
- Airway ClearanceДокумент24 страницыAirway ClearanceGoddy ManzanoОценок пока нет
- Tracheostomy Care: Thanuja Eleena MathewДокумент20 страницTracheostomy Care: Thanuja Eleena MathewOng Karl100% (3)
- TracheostomyДокумент28 страницTracheostomyprivatejarjarbinksОценок пока нет
- Trends in Anaesthesia and Critical Care: Brendan A. Mcgrath, Daniel HaleyДокумент3 страницыTrends in Anaesthesia and Critical Care: Brendan A. Mcgrath, Daniel HaleyRima RaisyiahОценок пока нет
- Closure of Paediatric Tracheocutaneous Fistula - Surgical TechniqueДокумент6 страницClosure of Paediatric Tracheocutaneous Fistula - Surgical Techniquehai1Оценок пока нет
- Tracheostomy CareДокумент15 страницTracheostomy CareZabeth ZabОценок пока нет
- TracheotomyДокумент4 страницыTracheotomyWilma VeniaОценок пока нет
- Skills PrelimДокумент24 страницыSkills PrelimBrent Ouen C. PenuelaОценок пока нет
- TEST BANK Chapter 21Документ6 страницTEST BANK Chapter 21Louise Lorraine TaculodОценок пока нет
- NAP4 Summary SheetДокумент1 страницаNAP4 Summary SheetAnonymous w4lLoMd7Оценок пока нет
- Nursing Performance Checklist TracheostomyДокумент3 страницыNursing Performance Checklist TracheostomySyahrilKiyai100% (1)
- Marshwood 3-17-20 Statement of DeficienciesДокумент17 страницMarshwood 3-17-20 Statement of DeficienciesMaine Trust For Local NewsОценок пока нет
- Intraoperative Airway Management Considerations.11Документ9 страницIntraoperative Airway Management Considerations.11anne di donatoОценок пока нет
- Non Invasive VentilationДокумент58 страницNon Invasive VentilationsachinОценок пока нет
- Executive Summary of UPenn OMFS Covid Conference - Indrakanti PDFДокумент8 страницExecutive Summary of UPenn OMFS Covid Conference - Indrakanti PDFasda201487Оценок пока нет
- Portex Sterile Nasopharyngeal AirwayДокумент5 страницPortex Sterile Nasopharyngeal AirwayRizka FadilahОценок пока нет
- ICU Lines TubesДокумент7 страницICU Lines TubesCindy MurphyОценок пока нет
- Timing of Tracheostomy For Prolonged Respiratory Wean in Critically Ill Coronavirus Disease 2019 Patients A Machine Learning ApproachДокумент9 страницTiming of Tracheostomy For Prolonged Respiratory Wean in Critically Ill Coronavirus Disease 2019 Patients A Machine Learning ApproachDewa OkaОценок пока нет
- Chapter 22 Upper Respiratory DisorderДокумент171 страницаChapter 22 Upper Respiratory DisorderAnnette Aquino GuevarraОценок пока нет
- Tracheostomy: Presented By: Barte, Hannah Aida D. Balamurugan, RameebhaДокумент21 страницаTracheostomy: Presented By: Barte, Hannah Aida D. Balamurugan, RameebhaThakoon Tts100% (1)
- Tracheal Intubation in Critical Ill Patient PDFДокумент8 страницTracheal Intubation in Critical Ill Patient PDFArdi FkuiОценок пока нет
- Pepp Renewal ManualДокумент21 страницаPepp Renewal ManualRaquel ReisОценок пока нет
- Applied Nursing ResearchДокумент5 страницApplied Nursing Researchfluffy4202011Оценок пока нет
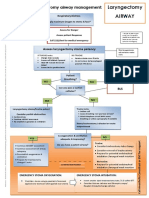
- Laryngectomy Airway: Emergency Tracheostomy Airway ManagementДокумент1 страницаLaryngectomy Airway: Emergency Tracheostomy Airway ManagementDana IlieОценок пока нет
- Airway ManagementДокумент13 страницAirway ManagementAlaa DaoudОценок пока нет
- Ent Osce - UpdatedДокумент24 страницыEnt Osce - UpdatedHoney100% (1)
- 2019 ALS 1 Manual V4 FinalДокумент53 страницы2019 ALS 1 Manual V4 FinalyusupОценок пока нет
- 11.1 Diagnosis and Management of Surgical Complications-Dr. Naui (Kimi Ledda)Документ10 страниц11.1 Diagnosis and Management of Surgical Complications-Dr. Naui (Kimi Ledda)Myrtle Yvonne RagubОценок пока нет
- SpringhДокумент22 страницыSpringhMary Hiromi MizushimaОценок пока нет