Вам также может понравиться
- EFT GuideДокумент11 страницEFT Guidenokaion19% (26)
- Introduction To Occupational Therapy PDFДокумент291 страницаIntroduction To Occupational Therapy PDFMurat Hasan BaşaranОценок пока нет
- Substance Use DisordersДокумент28 страницSubstance Use DisordersAbdul NazarОценок пока нет
- Interview: Patient HistoryДокумент8 страницInterview: Patient HistoryquelspectacleОценок пока нет
- Evidence-Based Practice in Pediatric Physical Therapy by BarryДокумент14 страницEvidence-Based Practice in Pediatric Physical Therapy by BarryFe TusОценок пока нет
- SR - Hse Officer (8104)Документ5 страницSR - Hse Officer (8104)Nijo Joseph100% (1)
- Psychodiagnostics and Psychological AssessmentДокумент4 страницыPsychodiagnostics and Psychological AssessmentBim arra0% (1)
- Teenage AnxietyДокумент34 страницыTeenage Anxietyamit100% (1)
- An Assessment of Five (PANSS, SAPS, SANS, NSA-16, CGI-SCH) CommonlyДокумент7 страницAn Assessment of Five (PANSS, SAPS, SANS, NSA-16, CGI-SCH) Commonlysyarifah husna100% (1)
- History Taking and Mental State Examination 2Документ35 страницHistory Taking and Mental State Examination 2Noreen Choudhri100% (2)
- List of DisordersДокумент4 страницыList of DisordersRain Simonette GuanОценок пока нет
- Hostility InventoryДокумент2 страницыHostility InventoryMeyrick AbreuОценок пока нет
- A Case Study of Generalized Anxiety DisorderДокумент10 страницA Case Study of Generalized Anxiety DisorderRina PerezОценок пока нет
- Pediatrics: St. Elizabeth Family Medicine Residency ProgramДокумент9 страницPediatrics: St. Elizabeth Family Medicine Residency Programwingchun108tekОценок пока нет
- 1999 Aversion Therapy-BEДокумент6 страниц1999 Aversion Therapy-BEprabhaОценок пока нет
- Treatment Modalities For Mood DisordersДокумент55 страницTreatment Modalities For Mood DisordersGlory MimiОценок пока нет
- k18 - Senior - Psychiatric EmergencyДокумент57 страницk18 - Senior - Psychiatric EmergencyZikri Putra Lan LubisОценок пока нет
- Joshua Dodot Case StudyДокумент2 страницыJoshua Dodot Case StudyJoshua Ringor100% (1)
- Postpartum Psychosis: Clinical Considerations: Marlene Freeman, M.DДокумент9 страницPostpartum Psychosis: Clinical Considerations: Marlene Freeman, M.DKreshnik IdrizajОценок пока нет
- Methods of TherapyДокумент6 страницMethods of TherapyRomeliza Ann Dela CruzОценок пока нет
- Imagery CBTДокумент3 страницыImagery CBTMichelle YongОценок пока нет
- DBT ReviewДокумент34 страницыDBT ReviewMariel SalgadoОценок пока нет
- Introduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPДокумент33 страницыIntroduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPSachiko Yosores100% (1)
- Wilson - Treatmen of Binge Eating Disorder PDFДокумент11 страницWilson - Treatmen of Binge Eating Disorder PDFGustavo AyalaОценок пока нет
- UW Notes - 13 - PsychiatryДокумент21 страницаUW Notes - 13 - PsychiatryDor BenayounОценок пока нет
- APA Citations For Nursing TextbooksДокумент1 страницаAPA Citations For Nursing Textbooksbbianca199075% (4)
- Bipolar Depression/Mania: SKINNY ReasoningДокумент9 страницBipolar Depression/Mania: SKINNY ReasoningSharon TanveerОценок пока нет
- Emotional Competence: The Fountain of personal, professional and private SuccessОт EverandEmotional Competence: The Fountain of personal, professional and private SuccessОценок пока нет
- Psychiatry Info - FinalДокумент8 страницPsychiatry Info - FinalH_QasimОценок пока нет
- Anxiety DisordersДокумент7 страницAnxiety Disorderssuresh patilОценок пока нет
- Zung Self-Rating Anxiety ScaleДокумент2 страницыZung Self-Rating Anxiety ScaleAbdur RahmanОценок пока нет
- Lecture 9. Special Care - Terminal & Palliative CareДокумент25 страницLecture 9. Special Care - Terminal & Palliative CareAnn Heerah100% (1)
- Notes: Customer EmotionsДокумент2 страницыNotes: Customer EmotionsNageshwar YadavОценок пока нет
- Anxiety DisordersДокумент18 страницAnxiety DisordersAzahed ArturoОценок пока нет
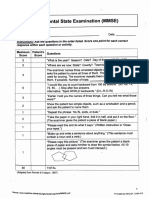
- Mini-Mental State Examination (MMSE)Документ3 страницыMini-Mental State Examination (MMSE)Prescilla San PedroОценок пока нет
- Jurnal BipolarДокумент11 страницJurnal BipolarRihan Hanri100% (1)
- Comprehensive Exam in Nursing Part 2Документ41 страницаComprehensive Exam in Nursing Part 2Ariane-Gay Cristobal DuranОценок пока нет
- BDDQДокумент1 страницаBDDQvaradh24Оценок пока нет
- 6 Surprising Habits That Hurt His Sex LifeДокумент7 страниц6 Surprising Habits That Hurt His Sex LifeBhagoo Hathey100% (1)
- Stress &healthДокумент18 страницStress &healthsatmayaniОценок пока нет
- Mental Health Through Forgiveness Exploring The Roots and Benefits PDFДокумент16 страницMental Health Through Forgiveness Exploring The Roots and Benefits PDFshindyОценок пока нет
- Teacher EducationДокумент32 страницыTeacher Educationsoumya satheshОценок пока нет
- What? Me Worry!?! What? Me Worry!?!Документ7 страницWhat? Me Worry!?! What? Me Worry!?!KonkmanОценок пока нет
- ISST May 2015 Schema Therapy BulletinДокумент18 страницISST May 2015 Schema Therapy Bulletinxx xxОценок пока нет
- Multimodal Therapy FinalДокумент26 страницMultimodal Therapy Finalkousalyasivakumaran1503100% (1)
- PSYCH - PsychosomaticdelasalleДокумент58 страницPSYCH - Psychosomaticdelasalleapi-3856051100% (1)
- PTSDДокумент17 страницPTSDadrianaОценок пока нет
- Terminology of PsychiatryДокумент6 страницTerminology of PsychiatryHassan.shehri100% (1)
- Test Personal It AteДокумент9 страницTest Personal It AteMihaela Sindie0% (1)
- A015 CopilulsimptomatologieДокумент21 страницаA015 CopilulsimptomatologieOana VezanОценок пока нет
- Personality Traits and Anxiety SymptomsДокумент19 страницPersonality Traits and Anxiety SymptomsSusana Díaz100% (1)
- Milieu MGT & Group TherapyДокумент28 страницMilieu MGT & Group TherapyGlory MimiОценок пока нет
- Grief and Loss: Author: DR Ofra FriedДокумент3 страницыGrief and Loss: Author: DR Ofra FriedFayasulhusain MuthalibОценок пока нет
- Shalit - Efficiency of PsychotherapyДокумент9 страницShalit - Efficiency of PsychotherapyAyerevОценок пока нет
- Mental Status ExaminationДокумент7 страницMental Status ExaminationChristine MatasОценок пока нет
- Rachman 1993Документ10 страницRachman 1993affcadvОценок пока нет
- Impactul Profilului Actiunii Pe Receptori A Antipsihoticelor Tipice Si Atipice În TratamentulДокумент10 страницImpactul Profilului Actiunii Pe Receptori A Antipsihoticelor Tipice Si Atipice În TratamentulAlina VeraОценок пока нет
- Presentation FAMILY THERAPYДокумент51 страницаPresentation FAMILY THERAPYAnjan Dhakal100% (1)
- 1 2018Документ48 страниц1 2018Lizz22Оценок пока нет
- Mood DisordersДокумент6 страницMood Disordersapi-217446206Оценок пока нет
- Podcast Anxiety and DepressionДокумент5 страницPodcast Anxiety and DepressionSyifa Olyfiani SariОценок пока нет
- Csep-II Experiential Therapy Session FormДокумент16 страницCsep-II Experiential Therapy Session FormSicologo Felipe PuertaОценок пока нет
- Research Article: Emotion Regulation Predicts Anxiety Over A Five-Year Interval: A Cross-Lagged Panel AnalysisДокумент10 страницResearch Article: Emotion Regulation Predicts Anxiety Over A Five-Year Interval: A Cross-Lagged Panel AnalysismargauxchenОценок пока нет
- Lifestyle Assessment FormДокумент17 страницLifestyle Assessment FormMarina SwansonОценок пока нет
- Transcending Bipolar Disorder: My Own True Story of Recovery from Mental IllnessОт EverandTranscending Bipolar Disorder: My Own True Story of Recovery from Mental IllnessОценок пока нет
- Pappas Bikhazi 2023 Babe Ruth S Anaplastic Epidermoid Carcinoma of The NasopharynxДокумент5 страницPappas Bikhazi 2023 Babe Ruth S Anaplastic Epidermoid Carcinoma of The NasopharynxVinoster ProductionОценок пока нет
- Dibasic Sodium PhosphateДокумент0 страницDibasic Sodium PhosphateWilliam ChandraОценок пока нет
- J Villanueva Group 2Документ22 страницыJ Villanueva Group 2Caryl Jole PaligsaОценок пока нет
- AWB Health Care PDFДокумент54 страницыAWB Health Care PDFimepsystemsОценок пока нет
- Assess PDFДокумент9 страницAssess PDFJov'z GuerreroОценок пока нет
- Maharashtra Public Service Commission Maharashtra Subordinate Services Main Examination - 2019Документ59 страницMaharashtra Public Service Commission Maharashtra Subordinate Services Main Examination - 2019S KatyarmalОценок пока нет
- Set C QP Eng Xii 23-24Документ11 страницSet C QP Eng Xii 23-24mafiajack21Оценок пока нет
- Job Chart of Physical Education Teachers - AP GOVTДокумент3 страницыJob Chart of Physical Education Teachers - AP GOVTRamachandra Rao100% (1)
- Medieval BodiesДокумент2 страницыMedieval BodiesKoh Yen SinОценок пока нет
- CephalosporinsДокумент20 страницCephalosporinsBianca Andrea RagazaОценок пока нет
- Components of Fitness, PARQ and TestingДокумент29 страницComponents of Fitness, PARQ and TestingLynОценок пока нет
- RISK ASSESSMENT REPORT - George Municipality - Tender ENG0042016 Installation of Perimeter Concrete Palisade FeДокумент10 страницRISK ASSESSMENT REPORT - George Municipality - Tender ENG0042016 Installation of Perimeter Concrete Palisade FeemmyОценок пока нет
- Topic ListДокумент6 страницTopic ListEdwinОценок пока нет
- Quadruple Aim in HealthcareДокумент2 страницыQuadruple Aim in HealthcareMarimiel PagulayanОценок пока нет
- Asa PSC System PDFДокумент2 страницыAsa PSC System PDFKen WonОценок пока нет
- Blood and Tissue Flagellates BSCДокумент27 страницBlood and Tissue Flagellates BSCSisay FentaОценок пока нет
- Typology of Nursing Problems in Family Nursing PracticeДокумент4 страницыTypology of Nursing Problems in Family Nursing PracticeLeah Abdul KabibОценок пока нет
- Group DR - Script - Allergic Rhinitis (Peanut Allergy) Health EducationДокумент10 страницGroup DR - Script - Allergic Rhinitis (Peanut Allergy) Health EducationKyra Bianca R. FamacionОценок пока нет
- Polytechnic of Health Denpasar Is An Institution of Higher Education Official of The Department of Health Which Is The Technical Implementation UnitДокумент1 страницаPolytechnic of Health Denpasar Is An Institution of Higher Education Official of The Department of Health Which Is The Technical Implementation UnitDewi PradnyaniОценок пока нет
- Written Assignment Principles of Applied RehabilitationДокумент17 страницWritten Assignment Principles of Applied RehabilitationRuqaiyah RahmanОценок пока нет
- CV Petrangolini enДокумент8 страницCV Petrangolini enTeresa PetrangoliniОценок пока нет
- Effects of Mobile Games On The Academic Performance of Grade 12 StudentsДокумент6 страницEffects of Mobile Games On The Academic Performance of Grade 12 Studentsnichole romeroОценок пока нет
- NIH Public Access: Author ManuscriptДокумент17 страницNIH Public Access: Author ManuscriptJoyBoyXОценок пока нет