Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Accessory TragusДокумент3 страницыAccessory TragusDeba P SarmaОценок пока нет
- Acantholytic Solar Keratosis, M 67, Forehead PDFДокумент6 страницAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaОценок пока нет
- Pilar Cyst With CrystalsДокумент2 страницыPilar Cyst With CrystalsDeba P SarmaОценок пока нет
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Документ3 страницыAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaОценок пока нет
- Acantholytic Actinic KeratosisДокумент4 страницыAcantholytic Actinic KeratosisDeba P SarmaОценок пока нет
- Acantholytic Dermatosis With DyskeratosisДокумент11 страницAcantholytic Dermatosis With DyskeratosisDeba P SarmaОценок пока нет
- Acantholytic Bullous DiseaseДокумент4 страницыAcantholytic Bullous DiseaseDeba P SarmaОценок пока нет
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmДокумент7 страницXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaОценок пока нет
- Acantholytic Acanthoma. M 60, ScrotumДокумент8 страницAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaОценок пока нет
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Документ6 страницBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaОценок пока нет
- Xanthogranuloma, M 30, Right ElbowДокумент4 страницыXanthogranuloma, M 30, Right ElbowDeba P SarmaОценок пока нет
- Results of Search in Google Scholar On 'Deba P Sarma'Документ28 страницResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaОценок пока нет
- Xanthogranuloma PPT DSДокумент9 страницXanthogranuloma PPT DSDeba P SarmaОценок пока нет
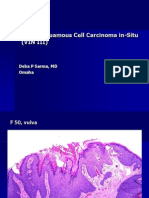
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaДокумент6 страницVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaОценок пока нет
- Verrucous Carcinoma of The Foot, M 63, Left FootДокумент8 страницVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
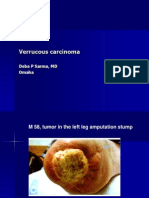
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpДокумент7 страницVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaОценок пока нет
- Verrucous Epidermal Nevus. F 43, ScalpДокумент4 страницыVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaОценок пока нет
- Verruca Vulgaris., M 22.,PPTДокумент2 страницыVerruca Vulgaris., M 22.,PPTDeba P SarmaОценок пока нет
- Thesis Protocol Final PDFДокумент39 страницThesis Protocol Final PDFApratim Roy ChoudhuryОценок пока нет
- Neuroimaging Advances in Holoprosencephaly: Re Ning The Spectrum of The Midline MalformationДокумент13 страницNeuroimaging Advances in Holoprosencephaly: Re Ning The Spectrum of The Midline Malformationfamiliesforhope100% (1)
- Neuroimaging - Clinical ApplicationsДокумент590 страницNeuroimaging - Clinical ApplicationsIndera VyasОценок пока нет
- Pengantar Anatomi NBSДокумент65 страницPengantar Anatomi NBSHa HaОценок пока нет
- CHOICES Acronym LeukoencephalopathyДокумент15 страницCHOICES Acronym LeukoencephalopathyLucas MontanhaОценок пока нет
- Guide Questions For The Human Brain (Cerebrum and Diencephalon)Документ11 страницGuide Questions For The Human Brain (Cerebrum and Diencephalon)Derick JuanОценок пока нет
- CT Brain Part II-AnatomyДокумент65 страницCT Brain Part II-AnatomyXhenni XhenniОценок пока нет
- Managerial Accounting 6th Edition Wild Test BankДокумент25 страницManagerial Accounting 6th Edition Wild Test BankDavidGarciaerfq100% (62)
- Sindrome Cloccs RadiographicsДокумент20 страницSindrome Cloccs RadiographicsJEAN CARLOS GALLO VALVERDEОценок пока нет
- Cerebral Cortex and Higher Cortical FunctionsДокумент14 страницCerebral Cortex and Higher Cortical FunctionsAcid ManaОценок пока нет
- Basal GangliaДокумент29 страницBasal Gangliaapi-19916399Оценок пока нет
- Corpus Callosum Lipomas in Children: Original InvestigationДокумент4 страницыCorpus Callosum Lipomas in Children: Original InvestigationHILA GINAОценок пока нет
- Ischemic StrokeДокумент49 страницIschemic StrokeMirna Ayu Permata SariОценок пока нет
- 7.sex Differencies in Lateralisation in Animal BrainДокумент224 страницы7.sex Differencies in Lateralisation in Animal BrainIuliana OlteanuОценок пока нет
- Limb Apraxia: Cynthia Ochipa, Ph.D. and Leslie J. Gonzalez Rothi, PH.DДокумент8 страницLimb Apraxia: Cynthia Ochipa, Ph.D. and Leslie J. Gonzalez Rothi, PH.DbilljonestanawalОценок пока нет
- Sperry Roger Ecs 2003Документ7 страницSperry Roger Ecs 2003Johnmark ObligarОценок пока нет
- The Parallel Brain. The Cognitive Neuroscience of The Corpus CallosumДокумент581 страницаThe Parallel Brain. The Cognitive Neuroscience of The Corpus Callosumjuanete9Оценок пока нет
- Author 'S Accepted ManuscriptДокумент46 страницAuthor 'S Accepted ManuscriptRaul DoctoОценок пока нет
- 100 Anatomy MCQДокумент19 страниц100 Anatomy MCQsudheerbds63690% (10)
- Malignant Gliomas - A Case StudyДокумент181 страницаMalignant Gliomas - A Case StudyJay-Anne Amor CasiaОценок пока нет
- Normal Mri Brain - Dr. Piyush OjhaДокумент111 страницNormal Mri Brain - Dr. Piyush OjhaAndrada CatrinoiuОценок пока нет
- Neuromythology of EINSTEIN BriainДокумент5 страницNeuromythology of EINSTEIN BriainrorozainosОценок пока нет
- MCQ Anatomy Midyear 2016Документ78 страницMCQ Anatomy Midyear 2016Hager AbosalemОценок пока нет
- White MatterДокумент19 страницWhite MatterZoya MoraniОценок пока нет
- Apraxia, Agnosia and Disconnection SyndromesДокумент65 страницApraxia, Agnosia and Disconnection SyndromesDhawal Narang100% (1)
- Sectional Anatomy Sectional AnatomyДокумент34 страницыSectional Anatomy Sectional Anatomysyafiqa abdullahОценок пока нет
- Epilepsy and Brain LesionДокумент9 страницEpilepsy and Brain LesionPosadasLoezaJosueKarlaОценок пока нет
- Brain Left and Right Hemisphere PPT PresentationДокумент10 страницBrain Left and Right Hemisphere PPT PresentationAnushka Ridhi HiraОценок пока нет
- c3 - Dezvoltarea CreieruluiДокумент17 страницc3 - Dezvoltarea CreieruluiElena-Andreea MutОценок пока нет