Вам также может понравиться
- J. Biol. Chem.-2004-Pell-9597-605Документ10 страницJ. Biol. Chem.-2004-Pell-9597-605Kedar SharmaОценок пока нет
- Coot TutorialДокумент17 страницCoot TutorialKedar SharmaОценок пока нет
- Day1 Autodock PresentationДокумент21 страницаDay1 Autodock PresentationKedar SharmaОценок пока нет
- DNA Restriction Fragment Analysis & SequencingДокумент5 страницDNA Restriction Fragment Analysis & SequencingKedar SharmaОценок пока нет
- Gate 2006 PDFДокумент6 страницGate 2006 PDFKedar SharmaОценок пока нет
- BSMSThesis FisherДокумент49 страницBSMSThesis FisherKedar SharmaОценок пока нет
- Polymerase Chain ReactionДокумент25 страницPolymerase Chain ReactionKedar SharmaОценок пока нет
- Subject: Biology (Instructions) : Tata Institute of Fundamental Research Gs2010 Nationwide Dbs/Ncbs Written TestДокумент15 страницSubject: Biology (Instructions) : Tata Institute of Fundamental Research Gs2010 Nationwide Dbs/Ncbs Written TestRahul PatelОценок пока нет
- Grassroots Academy GATE-BIOTECH 2010 CorrespondenceДокумент8 страницGrassroots Academy GATE-BIOTECH 2010 CorrespondenceKedar SharmaОценок пока нет
- Anatomy & Physiology - The Spinal CordДокумент3 страницыAnatomy & Physiology - The Spinal CordKedar SharmaОценок пока нет
- CSIR-NET Cell Biology NotesДокумент32 страницыCSIR-NET Cell Biology NotesSrinivas Nakka100% (1)
- Dept. of Management Studies: Presentation byДокумент25 страницDept. of Management Studies: Presentation byKedar SharmaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
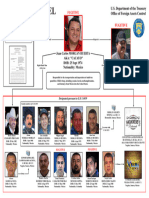
- Sinaloa ChartДокумент1 страницаSinaloa ChartJoel CanoОценок пока нет
- William's helpful backpackДокумент1 страницаWilliam's helpful backpackEnrique RodriguezОценок пока нет
- Professional Goals Plan 1 1Документ5 страницProfessional Goals Plan 1 1api-297284721Оценок пока нет
- OETC-HSE-O-EIR-F-000 Format Emissionsd To AirДокумент6 страницOETC-HSE-O-EIR-F-000 Format Emissionsd To AirMobin Thomas AbrahamОценок пока нет
- BHF CVD Statistics Global FactsheetДокумент12 страницBHF CVD Statistics Global FactsheetRobby Paguh TariganОценок пока нет
- Foai Fda PDFДокумент3 страницыFoai Fda PDFMadhuriОценок пока нет
- File Jurnal Infeksi NosokomialДокумент12 страницFile Jurnal Infeksi Nosokomialirmayani channelОценок пока нет
- Endocrine System PhysiologyДокумент2 страницыEndocrine System PhysiologyLuisGabitoОценок пока нет
- Ahmed Magdy Hatata - Strategic Marketing AssignmentДокумент12 страницAhmed Magdy Hatata - Strategic Marketing AssignmentAhmed HatataОценок пока нет
- Risk Assessment Palm Food FEDIOL Final 160522Документ18 страницRisk Assessment Palm Food FEDIOL Final 160522Jayashri chitteОценок пока нет
- VND - Openxmlformats Officedocument - Wordprocessingml.document&rendition 1 1Документ16 страницVND - Openxmlformats Officedocument - Wordprocessingml.document&rendition 1 1Umesh GawaliОценок пока нет
- Early Childhood Relationships ID: Pleasure Neurotic Anxiety EGO: Reality Decision-Maker SUPEREGO: Morality Moral AnxietyДокумент10 страницEarly Childhood Relationships ID: Pleasure Neurotic Anxiety EGO: Reality Decision-Maker SUPEREGO: Morality Moral AnxietyHannah RealuyoОценок пока нет
- Top 5 Online High School InternshipsДокумент2 страницыTop 5 Online High School InternshipsAzneef Ahammed Chowdury100% (1)
- Checklist of Mandatory Documentation Required by ISO 13485:2016Документ15 страницChecklist of Mandatory Documentation Required by ISO 13485:2016Ricky Mark100% (2)
- Arm - Unit 1 - Overview of ResearchДокумент23 страницыArm - Unit 1 - Overview of ResearchIvaturiAnithaОценок пока нет
- Ace Hot Work Permit Application Form PDFДокумент3 страницыAce Hot Work Permit Application Form PDFkevin100% (1)
- MultiSport-Mojo Training-Plan Marathon Advanced-3PRBM 16-Weeks Off-Sun FINALДокумент3 страницыMultiSport-Mojo Training-Plan Marathon Advanced-3PRBM 16-Weeks Off-Sun FINALJohn HTОценок пока нет
- Insight222 Research People Analytics Trends 2022 Impacting Business ValueДокумент44 страницыInsight222 Research People Analytics Trends 2022 Impacting Business ValueCCV CCVОценок пока нет
- Unit Proposal PresentationДокумент29 страницUnit Proposal PresentationRachel CortezОценок пока нет
- PE4 Mod1Документ16 страницPE4 Mod1wencylle casilОценок пока нет
- Essential Communication Skills For Conflict ResolutionДокумент15 страницEssential Communication Skills For Conflict Resolutionsoulinthone vilayphanhОценок пока нет
- BING Covid-19Документ9 страницBING Covid-19tirsha tjowasiОценок пока нет
- The History and Culture of Japanese FoodДокумент284 страницыThe History and Culture of Japanese FoodDiana67% (6)
- A.Haleem (2020) Areas of Academic Research With The Impact of COVID-19Документ8 страницA.Haleem (2020) Areas of Academic Research With The Impact of COVID-19Azizan RamlyОценок пока нет
- Red Cross Psychological First Aid BookДокумент28 страницRed Cross Psychological First Aid BookQuique ParadaОценок пока нет
- Characteristics of IOДокумент5 страницCharacteristics of IOLynzae100% (2)
- 5S: The Secret to Japanese SuccessДокумент39 страниц5S: The Secret to Japanese SuccessNerizza SomeraОценок пока нет
- Wheaters Basic Pathology A Text Atlas and Review of Histopathology 5th Edition Young Test BankДокумент5 страницWheaters Basic Pathology A Text Atlas and Review of Histopathology 5th Edition Young Test BankNicoleRoweanbtc100% (15)
- Study Of Mobile Data Consumption Of Management Student in Social MediaДокумент12 страницStudy Of Mobile Data Consumption Of Management Student in Social MediaShubham MeshramОценок пока нет
- Feasibility of Screening For Preschool Behavioral and Emotional Problems in Primary Care Using The Early Childhood Screening AssessmentДокумент9 страницFeasibility of Screening For Preschool Behavioral and Emotional Problems in Primary Care Using The Early Childhood Screening AssessmentAhmed RamzyОценок пока нет