Вам также может понравиться
- Psychiatry 2016Документ136 страницPsychiatry 2016Firas KОценок пока нет
- Disorders of Thought and SpeechДокумент50 страницDisorders of Thought and SpeechTilarupa BhattaraiОценок пока нет
- Delusion and HallucinationДокумент4 страницыDelusion and HallucinationRiezky FebriyantiОценок пока нет
- 1975 Conrad Imposture As A DefenseДокумент18 страниц1975 Conrad Imposture As A DefenseKevin McInnesОценок пока нет
- Major Tenets of TranscendentalismДокумент4 страницыMajor Tenets of TranscendentalismYam MarieОценок пока нет
- Chapter 11 Skill Development Exercise Handling GrievancesДокумент10 страницChapter 11 Skill Development Exercise Handling GrievancesMushira AnsariОценок пока нет
- Coexistence of Folie Communique e and Folie SimultaneeДокумент4 страницыCoexistence of Folie Communique e and Folie SimultaneeAna Rosa González Barroso0% (1)
- Epilepsy, Hysteria, and Neurasthenia by Briggs, Isaac G.Документ98 страницEpilepsy, Hysteria, and Neurasthenia by Briggs, Isaac G.Gutenberg.orgОценок пока нет
- Hypnosis As An Adjunct To CBT 1995Документ7 страницHypnosis As An Adjunct To CBT 1995MiguelAngelBrocОценок пока нет
- Dissociative Identity DisorderДокумент42 страницыDissociative Identity DisorderGsdhdbОценок пока нет
- Psych 9 (Signs and Symptoms)Документ5 страницPsych 9 (Signs and Symptoms)2013SecBОценок пока нет
- Barton - 1994 - Chaos, Self-Organization, and Psychology PDFДокумент10 страницBarton - 1994 - Chaos, Self-Organization, and Psychology PDFYesimОценок пока нет
- History Psychiatry ANAMNESISДокумент21 страницаHistory Psychiatry ANAMNESISDr. BrainОценок пока нет
- DrowningДокумент26 страницDrowningCristina L. JaysonОценок пока нет
- Module C Psychotic DifferentialДокумент11 страницModule C Psychotic Differentialark1974Оценок пока нет
- Major Depression With Psychotic FeaturesДокумент12 страницMajor Depression With Psychotic FeaturesNICOLE BASEОценок пока нет
- Pseudo HallucinationДокумент7 страницPseudo HallucinationAnonymous gUjimJKОценок пока нет
- Pitutary GlandДокумент3 страницыPitutary GlandMariannОценок пока нет
- 5momentsHandHygiene A3 PDFДокумент1 страница5momentsHandHygiene A3 PDFDwi SurantoОценок пока нет
- Chaos, Cognition and Disordered BrainДокумент4 страницыChaos, Cognition and Disordered BrainluisОценок пока нет
- Moon and Madness Reconsidered PDFДокумент8 страницMoon and Madness Reconsidered PDFvincentbracq100% (1)
- Meyer - Psychological Testing and Psychological AssessmentДокумент38 страницMeyer - Psychological Testing and Psychological AssessmentSpikeThePenguin100% (1)
- PsychiatryДокумент23 страницыPsychiatryNaveenKumarОценок пока нет
- Hysteria NeurosisДокумент19 страницHysteria NeurosisMonikaОценок пока нет
- Depression PsychoticДокумент10 страницDepression Psychoticharumimiaomiao_198930% (1)
- The Phenomenology of Intersubjectivity in Bipolar Disorder and SquizophreniaДокумент9 страницThe Phenomenology of Intersubjectivity in Bipolar Disorder and Squizophreniajanettst2Оценок пока нет
- Status AsthmaticusДокумент6 страницStatus AsthmaticusMae Azores100% (1)
- Understanding Epilepsy and Its Homeopathic AnswerДокумент21 страницаUnderstanding Epilepsy and Its Homeopathic AnswerDr. Sandeep Anwane100% (3)
- Schizophernia - Unit 1Документ15 страницSchizophernia - Unit 119PSY05 ATULYA VENKATESHОценок пока нет
- Kosadinos E, Who Is Afraid of Atypical Depression, Dubrovnik 2008Документ17 страницKosadinos E, Who Is Afraid of Atypical Depression, Dubrovnik 2008Emmanuel Manolis KosadinosОценок пока нет
- Psychiatry - A Text-Book For Students and Physicians - Stewart Paton. MD (1905) - BW PDFДокумент670 страницPsychiatry - A Text-Book For Students and Physicians - Stewart Paton. MD (1905) - BW PDFAbram KimОценок пока нет
- Dissociative Disorders - RamanДокумент14 страницDissociative Disorders - Ramanraman.pОценок пока нет
- Manic Depressive PsychosisДокумент2 страницыManic Depressive PsychosisAzmat Hussain Shah NaqviОценок пока нет
- CRVS HANDBOOK FOR HEALTH WORKERS (Second Edition)Документ159 страницCRVS HANDBOOK FOR HEALTH WORKERS (Second Edition)Jomer GonzalesОценок пока нет
- Definition of Normality and AbnormalityДокумент9 страницDefinition of Normality and AbnormalityJas BОценок пока нет
- Free Radical Theory of AgingДокумент2 страницыFree Radical Theory of AgingJenny Rose Colico RNОценок пока нет
- Control of Sleep and WakefulnessДокумент101 страницаControl of Sleep and WakefulnessLevente BalázsОценок пока нет
- Scizophrenia NCPДокумент1 страницаScizophrenia NCPKholid Abu Mohammad AlfaizinОценок пока нет
- This Study Resource Was: Spinal Cord Injury Case StudyДокумент3 страницыThis Study Resource Was: Spinal Cord Injury Case StudyMiss GОценок пока нет
- Unit 7: Schizophrenia Spectrum and Other Psychotic DisordersДокумент31 страницаUnit 7: Schizophrenia Spectrum and Other Psychotic DisordershackersОценок пока нет
- Depression Powerpoint - 2Документ26 страницDepression Powerpoint - 2danyalОценок пока нет
- Phenomenology Schizophrenia and Gestalt PDFДокумент58 страницPhenomenology Schizophrenia and Gestalt PDFAmalia GonzalezОценок пока нет
- A Critique of The Dopamine Hypothesis of Schizophrenia and PsychosisДокумент12 страницA Critique of The Dopamine Hypothesis of Schizophrenia and PsychosisXaviОценок пока нет
- Nursing Reading On Spinal InjuryДокумент4 страницыNursing Reading On Spinal InjuryKristel Diane RidaoОценок пока нет
- Kring Abnormal Psychology Chapter 5 Mood Disorders NotesДокумент14 страницKring Abnormal Psychology Chapter 5 Mood Disorders NotesAnn Ross FernandezОценок пока нет
- PSYCHIATRY Classification of Psychiatric Disorder (Dr. Rosal)Документ11 страницPSYCHIATRY Classification of Psychiatric Disorder (Dr. Rosal)Valcrist BalderОценок пока нет
- HypochondriasisДокумент12 страницHypochondriasisVendi Cahyadi RiandikaОценок пока нет
- Ugst Who Am I Essay 1Документ2 страницыUgst Who Am I Essay 1api-481398974Оценок пока нет
- Psych Typical Manif 1Документ10 страницPsych Typical Manif 1Arfi FachrulОценок пока нет
- PSYCHIATRY INTERVIEW-history and MseДокумент10 страницPSYCHIATRY INTERVIEW-history and MsemartinОценок пока нет
- Case Study SchizophreniaДокумент4 страницыCase Study SchizophreniaCristelle Anne FranciscoОценок пока нет
- Pathophysiology of Schizophrenia: February 2014Документ24 страницыPathophysiology of Schizophrenia: February 2014Tuderici IoanaОценок пока нет
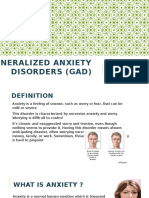
- Generalized Anxiety Disorders (GAD)Документ8 страницGeneralized Anxiety Disorders (GAD)Deasy Arindi PutriОценок пока нет
- Hopkins Symptom Checklist (HSCL-58) Derogatis1974Документ15 страницHopkins Symptom Checklist (HSCL-58) Derogatis1974MilosОценок пока нет
- Five Stages of GriefДокумент1 страницаFive Stages of GriefEsther CheongОценок пока нет
- A Case Report of Obsessive-Compulsive DisorderДокумент6 страницA Case Report of Obsessive-Compulsive DisorderfonsoalОценок пока нет
- Bortolotti 2018Документ19 страницBortolotti 2018José Eduardo PorcherОценок пока нет
- Psychiatric Nursing - Psycho PharmacologyДокумент50 страницPsychiatric Nursing - Psycho PharmacologyKaren MichelleОценок пока нет
- Schizophrenia Unmasked: Personal Stories and Proven Techniques to Reclaim Your LifeОт EverandSchizophrenia Unmasked: Personal Stories and Proven Techniques to Reclaim Your LifeОценок пока нет
- The Physiologic Basis and Clinical Applications of CryotherapyДокумент6 страницThe Physiologic Basis and Clinical Applications of CryotherapyomboОценок пока нет
- The Jail Report - Issue 203Документ20 страницThe Jail Report - Issue 203Andy Denton100% (1)
- (Grade 9) MAPEH (Health) - Drugs (2nd)Документ3 страницы(Grade 9) MAPEH (Health) - Drugs (2nd)KenОценок пока нет
- People vs. Anita Miranda Y BeltranДокумент2 страницыPeople vs. Anita Miranda Y BeltranMark Alexander FenidОценок пока нет
- XZXZДокумент4 страницыXZXZhenpupraОценок пока нет
- Methamphetamine 10Документ4 страницыMethamphetamine 10Teodora NeshovaОценок пока нет
- Amphetamines: Information For Health ProfessionalsДокумент12 страницAmphetamines: Information For Health ProfessionalsAsmaa LabibОценок пока нет
- UNC Meth Presentation 29oct2015 0Документ34 страницыUNC Meth Presentation 29oct2015 0JasonОценок пока нет
- Stnar34 MetanfetaminasДокумент88 страницStnar34 Metanfetaminashildana pachecoОценок пока нет
- METH PubSpeakДокумент9 страницMETH PubSpeakthehourofarrival100% (3)
- People v. OcfemiaДокумент2 страницыPeople v. OcfemiaNinaОценок пока нет
- Drug Addiction - NSTPДокумент9 страницDrug Addiction - NSTPRuvelyn NipasОценок пока нет
- D AbuseДокумент8 страницD AbuseFrancis AngtudОценок пока нет
- Module 6 - CwtsДокумент9 страницModule 6 - CwtsAmor Lisondra LegitimasОценок пока нет
- Guc 2773 59 32050 2023-05-10T08 57 49Документ22 страницыGuc 2773 59 32050 2023-05-10T08 57 49Hisham HusseinОценок пока нет
- Prep For JournalismДокумент135 страницPrep For JournalismMaxn ClairОценок пока нет
- Drug Education AND Vice ControlДокумент53 страницыDrug Education AND Vice ControlRizabel VillapandoОценок пока нет
- The Six Classifications of Drugs of AbuseДокумент2 страницыThe Six Classifications of Drugs of AbuseAnonymous EVihZ6Ts100% (2)
- True False Quiz Brochure 2013 PDFДокумент2 страницыTrue False Quiz Brochure 2013 PDFJahnna Marie PomaresОценок пока нет
- Lectures On Anti-Illegal DrugsДокумент67 страницLectures On Anti-Illegal DrugsNoli Narvadez0% (1)
- Substance Abuse Counseling Complete 5th EditionДокумент379 страницSubstance Abuse Counseling Complete 5th Editionnintendoagekid86% (59)
- Substance Abuse Beat 10 12 21Документ64 страницыSubstance Abuse Beat 10 12 21Mich GuarinoОценок пока нет
- NSTP ReviewerДокумент18 страницNSTP ReviewerKrystel TullaoОценок пока нет
- Drug Education and Vice Control: Compiled By: Kelvin P. SaludoДокумент46 страницDrug Education and Vice Control: Compiled By: Kelvin P. SaludoJARA, Joan M.Оценок пока нет
- Cold Cook Methods An Ethnographic Explor PDFДокумент11 страницCold Cook Methods An Ethnographic Explor PDFChad Conway43% (7)
- Don Honorio Ventura State University College of Education Bachelor of Physical EducationДокумент3 страницыDon Honorio Ventura State University College of Education Bachelor of Physical EducationPrinces YumulОценок пока нет
- Drugs Are Listed AlphabeticallyДокумент17 страницDrugs Are Listed AlphabeticallysyrieangelОценок пока нет
- Mi Pvs SCH Oz Phrenia 2019Документ21 страницаMi Pvs SCH Oz Phrenia 2019Jamison ParfittОценок пока нет
- NSTP ReviewerДокумент13 страницNSTP ReviewerPamela Isabelle April EncenzoОценок пока нет
- Breaking Bad TeaserДокумент3 страницыBreaking Bad Teaserjorge escobarОценок пока нет