Вам также может понравиться
- Holistic Baby Acupressure System: 12 Acupressure Points for Pediatric Sleep Improvement and Wellness SupportОт EverandHolistic Baby Acupressure System: 12 Acupressure Points for Pediatric Sleep Improvement and Wellness SupportОценок пока нет
- DR Case Presentation Group 1 PIHДокумент6 страницDR Case Presentation Group 1 PIHCharles Vergel Sabaldan MarceraОценок пока нет
- Case-3 Pedia AgeДокумент6 страницCase-3 Pedia AgeCharlie65129Оценок пока нет
- Makalah Ce Carissa - 18.08.2020 PK 18.26Документ75 страницMakalah Ce Carissa - 18.08.2020 PK 18.26sumbiaindrianiОценок пока нет
- En MB Sukma 11 Dec 18 13.10Документ35 страницEn MB Sukma 11 Dec 18 13.10Handoyo KooОценок пока нет
- OBS Case Report 1Документ12 страницOBS Case Report 1Rikoy ArikarОценок пока нет
- Case 3 and 4Документ9 страницCase 3 and 4Jethro Floyd QuintoОценок пока нет
- Hirschsprung'S Disease in A Child: Case ReportДокумент57 страницHirschsprung'S Disease in A Child: Case ReportHans NatanaelОценок пока нет
- Block 7 Active Phase 1st Stage of LaborДокумент29 страницBlock 7 Active Phase 1st Stage of LaborRoselle Joy D. RosalejosОценок пока нет
- PP Type Ii AnteriorДокумент10 страницPP Type Ii AnteriorAiman ArifinОценок пока нет
- Hypokalemia Periodic ParalysisДокумент14 страницHypokalemia Periodic ParalysisJennirose JingОценок пока нет
- Case Study CSДокумент21 страницаCase Study CSThessa Lonica GarciaОценок пока нет
- Case Write Up 2Документ16 страницCase Write Up 2Shidev100% (1)
- Cwu O&g 1 PPROMДокумент13 страницCwu O&g 1 PPROMFaris Mohd Nasir100% (1)
- Foreign Body AspirationДокумент4 страницыForeign Body AspirationpriscaОценок пока нет
- Intrapartum Complication: Shoulder DystociaДокумент4 страницыIntrapartum Complication: Shoulder DystociaRIECHELLE SEVILLAОценок пока нет
- Case Press Ob WardДокумент9 страницCase Press Ob Wardjohn castroОценок пока нет
- Case Pre EditedДокумент112 страницCase Pre EditedZanesville Lymont L. SubidoОценок пока нет
- College of Nursing: Panpacific University North PhilippinesДокумент20 страницCollege of Nursing: Panpacific University North PhilippinesMar OrdanzaОценок пока нет
- Case Presentation FinalДокумент22 страницыCase Presentation Finalmafi0914Оценок пока нет
- Obstetrics and Gynaecology Write Up 3Документ10 страницObstetrics and Gynaecology Write Up 3Luqman HarunОценок пока нет
- Pedia - DengueДокумент10 страницPedia - DengueJan Mikhail FrascoОценок пока нет
- Document 0730 PMДокумент9 страницDocument 0730 PMMelissa Aina Mohd YusofОценок пока нет
- PEDIA Case - Pneumonia 2 VSDДокумент17 страницPEDIA Case - Pneumonia 2 VSDGrace Antonette PatiОценок пока нет
- Postnatl Case StudyДокумент21 страницаPostnatl Case StudyRed Williams100% (4)
- OBGYN Vaginal Delivery DikaДокумент10 страницOBGYN Vaginal Delivery DikaOnyedika EgbujoОценок пока нет
- Incomplete Abortion PanggoДокумент20 страницIncomplete Abortion PanggoRoselle Joy D. RosalejosОценок пока нет
- Infeksionet e Traktit Urinar STUDIM RASTIДокумент15 страницInfeksionet e Traktit Urinar STUDIM RASTILindrit AliuОценок пока нет
- Acute Appendicitis Group CДокумент40 страницAcute Appendicitis Group CHeart TolenadaОценок пока нет
- Post DatismДокумент10 страницPost DatismAiman ArifinОценок пока нет
- Incomplete Miscarriage Finaliiiii 2.0Документ10 страницIncomplete Miscarriage Finaliiiii 2.0emmanuel oduОценок пока нет
- CWU 2 Epipepsy - West SyndromeДокумент10 страницCWU 2 Epipepsy - West SyndromeZul Hisyam Fikri100% (1)
- CASE STUDY (ABNORMAL PREGNANCY) .Edited (2)Документ9 страницCASE STUDY (ABNORMAL PREGNANCY) .Edited (2)niyoc68859Оценок пока нет
- Pregnancy Induced Hypertension (PIH) : Case Scenario 4Документ4 страницыPregnancy Induced Hypertension (PIH) : Case Scenario 4Mae Arra Lecobu-anОценок пока нет
- Case Report Due Date: 16 October 2020Документ10 страницCase Report Due Date: 16 October 2020TemahlungwaneОценок пока нет
- Obg - Case Presentation - FGRДокумент24 страницыObg - Case Presentation - FGRNazee NazreenОценок пока нет
- Pediatrics Preceptorial JuanitasMDДокумент5 страницPediatrics Preceptorial JuanitasMDCharles Jebb Belonio JuanitasОценок пока нет
- Post DateДокумент4 страницыPost DateRae RayОценок пока нет
- Case Study, g6Документ62 страницыCase Study, g6julie pearl peliyoОценок пока нет
- Preterm Breech Case StudyДокумент10 страницPreterm Breech Case StudyYa Mei LiОценок пока нет
- Patient Report. 2Документ7 страницPatient Report. 2Ahlam Azam, MohamedОценок пока нет
- Case Study On FCBDДокумент38 страницCase Study On FCBDKwinutskie LiteratoОценок пока нет
- Makalahkoheri 10:7:19Документ18 страницMakalahkoheri 10:7:19PutuIantaParamaSiwiОценок пока нет
- A Case Presentation In: Assigned Area: Ob Concept: "Care of Family and Family Health"Документ33 страницыA Case Presentation In: Assigned Area: Ob Concept: "Care of Family and Family Health"Maria Charis Anne IndananОценок пока нет
- Obstetric Nursing Care PlanДокумент12 страницObstetric Nursing Care PlanJass Mira Bueno100% (1)
- Cwu Ong TwinДокумент14 страницCwu Ong TwinAiman ArifinОценок пока нет
- Obstetric Nursing Care PlanДокумент12 страницObstetric Nursing Care PlanfiercesheОценок пока нет
- Pediatric Sample Case (Seizure) PDFДокумент8 страницPediatric Sample Case (Seizure) PDFIvan RoiОценок пока нет
- Nursing Health History: Homework HelpДокумент12 страницNursing Health History: Homework HelplicservernoidaОценок пока нет
- MS GCS Cornual Ectopic PregnancyДокумент57 страницMS GCS Cornual Ectopic PregnancyCarelle Faith Serrano AsuncionОценок пока нет
- Patient ProfileДокумент3 страницыPatient ProfileKhaled GharaibehОценок пока нет
- GDM 3Документ12 страницGDM 3Aiman ArifinОценок пока нет
- OB Care Plan Obstetric Nursing Care Plan 1Документ25 страницOB Care Plan Obstetric Nursing Care Plan 1Gitanjali Singh PasiОценок пока нет
- I.I Biographic DataДокумент10 страницI.I Biographic DataRobby James RabeОценок пока нет
- Long Case - Susilowati (En Lokal)Документ17 страницLong Case - Susilowati (En Lokal)Hendra WardhanaОценок пока нет
- DR Case StudyДокумент3 страницыDR Case StudyMikaela Gabrielle GERALIОценок пока нет
- Essential HTN in PregnancyДокумент13 страницEssential HTN in PregnancyAiman ArifinОценок пока нет
- VacuumДокумент22 страницыVacuumRed WilliamsОценок пока нет
- Diarrhea of 1 Day Duration: Durante, Esperon, Espino, Fernando, Figuracion, Flores, Fong, Francisco JДокумент37 страницDiarrhea of 1 Day Duration: Durante, Esperon, Espino, Fernando, Figuracion, Flores, Fong, Francisco JMisheilPascuaОценок пока нет
- Individual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Документ2 страницыIndividual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Angelo VillafrancaОценок пока нет
- Amazon PrimeДокумент27 страницAmazon PrimeMohamedОценок пока нет
- The Java Collections Framework: InterfacesДокумент22 страницыThe Java Collections Framework: InterfacesSourav DasОценок пока нет
- Syntax 1Документ35 страницSyntax 1galcarolina722202100% (1)
- Gonzales v. PennisiДокумент15 страницGonzales v. Pennisimceline19Оценок пока нет
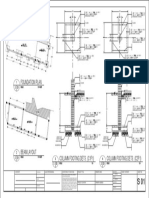
- Foundation Plan: Scale 1:100 MTSДокумент1 страницаFoundation Plan: Scale 1:100 MTSJayson Ayon MendozaОценок пока нет
- EBO Pipeline Process 7 23 04Документ4 страницыEBO Pipeline Process 7 23 04Kevin WrightОценок пока нет
- Dior Product Development PresentationДокумент59 страницDior Product Development PresentationSade WycheОценок пока нет
- Sales Manager Job DescriptionДокумент8 страницSales Manager Job Descriptionsalesmanagement264Оценок пока нет
- Harry Potter and The Prisoner of Azkaban: Chapter 3-1 Owl PostДокумент20 страницHarry Potter and The Prisoner of Azkaban: Chapter 3-1 Owl PostodfasdОценок пока нет
- Lease of Playground To A SchoolДокумент2 страницыLease of Playground To A SchoolSutapaОценок пока нет
- Technical Activities: Ken Goldberg, VP Technical Activities Spring 2007, ICRA, RomeДокумент52 страницыTechnical Activities: Ken Goldberg, VP Technical Activities Spring 2007, ICRA, RomeWasim Ahmad KhanОценок пока нет
- LTE Principle and LTE PlanningДокумент70 страницLTE Principle and LTE PlanningShain SalimОценок пока нет
- Tiktok, Identity Struggles and Mental Health Issues: How Are The Youth of Today Coping?Документ6 страницTiktok, Identity Struggles and Mental Health Issues: How Are The Youth of Today Coping?Trúc NgânОценок пока нет
- Grade Up CurrentsДокумент273 страницыGrade Up CurrentsAmiya RoyОценок пока нет
- Constantin Floros, Kenneth Chalmers - New Ears For New Music-Peter Lang GMBH, Internationaler Verlag Der Wissenschaften (2014)Документ242 страницыConstantin Floros, Kenneth Chalmers - New Ears For New Music-Peter Lang GMBH, Internationaler Verlag Der Wissenschaften (2014)paperocamillo100% (3)
- Syllabus Spring 2021Документ17 страницSyllabus Spring 2021Eden ParkОценок пока нет
- Assignment On How To Increase Own Brand Mantras: Submition Date: January 29,2021Документ5 страницAssignment On How To Increase Own Brand Mantras: Submition Date: January 29,2021Ferari DroboОценок пока нет
- Crimiology MCQ 2Документ15 страницCrimiology MCQ 2varunendra pandeyОценок пока нет
- Revalida ResearchДокумент3 страницыRevalida ResearchJakie UbinaОценок пока нет
- Week 4Документ5 страницWeek 4عبدالرحمن الحربيОценок пока нет
- Industrial Thread (Sewing Thread)Документ8 страницIndustrial Thread (Sewing Thread)sandhyaishtaОценок пока нет
- @PAKET A - TPM BAHASA INGGRIS KuДокумент37 страниц@PAKET A - TPM BAHASA INGGRIS KuRamona DessiatriОценок пока нет
- Nonviolent Communication Lessons 2-20-18Документ210 страницNonviolent Communication Lessons 2-20-18Ice George100% (1)
- Nail DisordersДокумент123 страницыNail DisordersyaraamadoОценок пока нет
- Snowman Card Game PDFДокумент2 страницыSnowman Card Game PDFFOAОценок пока нет
- Disruptive Strategy Final Paper Company ProfilesДокумент2 страницыDisruptive Strategy Final Paper Company ProfilesHumberto Jose Arias BarrosОценок пока нет
- 00664-Hepting Excerpts of RecordДокумент240 страниц00664-Hepting Excerpts of RecordlegalmattersОценок пока нет
- Proximity Principle of DesignДокумент6 страницProximity Principle of DesignSukhdeepОценок пока нет
- A Scale To Measure The Transformational Leadership of Extension Personnel at Lower Level of ManagementДокумент8 страницA Scale To Measure The Transformational Leadership of Extension Personnel at Lower Level of ManagementMohamed Saad AliОценок пока нет
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Рейтинг: 3 из 5 звезд3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 4.5 из 5 звезд4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (32)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 4 из 5 звезд4/5 (4)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (254)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (170)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesОт EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesРейтинг: 4.5 из 5 звезд4.5/5 (1412)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceОт EverandTo Explain the World: The Discovery of Modern ScienceРейтинг: 3.5 из 5 звезд3.5/5 (51)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (46)
- The Marshmallow Test: Mastering Self-ControlОт EverandThe Marshmallow Test: Mastering Self-ControlРейтинг: 4.5 из 5 звезд4.5/5 (60)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4.5 из 5 звезд4.5/5 (6)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingОт EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingРейтинг: 1 из 5 звезд1/5 (1)