Вам также может понравиться
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisОт EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisРейтинг: 5 из 5 звезд5/5 (1)
- NCMMSN Notes - Sacramento, Karl SebastianДокумент96 страницNCMMSN Notes - Sacramento, Karl SebastianRHEA MAY CAPORОценок пока нет
- Heart & Hemodynamics NotesДокумент8 страницHeart & Hemodynamics NotesBrandice BradleyОценок пока нет
- Cardiac Ana & DxticsДокумент3 страницыCardiac Ana & Dxticsjames garciaОценок пока нет
- Components of The Cardiovascular SystemДокумент23 страницыComponents of The Cardiovascular SystemMr. DummyОценок пока нет
- Structure and Function of The Cardiovascular System PDFДокумент9 страницStructure and Function of The Cardiovascular System PDFteuuuuОценок пока нет
- Heart Anatomy: LocationДокумент45 страницHeart Anatomy: LocationZaira100% (1)
- Lecture - 3 Properties of Cardiac MuscleДокумент35 страницLecture - 3 Properties of Cardiac MuscleMRM7MDОценок пока нет
- Cardiovascular Physical TherapyДокумент206 страницCardiovascular Physical TherapyJuanitoCabatañaLimIII100% (2)
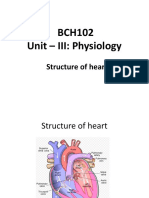
- Structure of the HeartДокумент17 страницStructure of the Heartdivya vajpayeeОценок пока нет
- EKG Study Guide RevisedДокумент29 страницEKG Study Guide Revisedflashyboy506Оценок пока нет
- TM 8 TM 8only Clinical Exam of Heart and Circulatory System AGWEnglishДокумент66 страницTM 8 TM 8only Clinical Exam of Heart and Circulatory System AGWEnglishcellin rubianti azzharaОценок пока нет
- Heart PathophysiologyДокумент20 страницHeart PathophysiologyDoctorDrapion100% (2)
- The HeartДокумент65 страницThe HeartMichael SamaniegoОценок пока нет
- Lesson 3Документ71 страницаLesson 3Angel joyce ValenciaОценок пока нет
- The Circulatory SystemДокумент25 страницThe Circulatory SystemEduardson PHОценок пока нет
- Anatomy and Physiology of The HeartДокумент9 страницAnatomy and Physiology of The HeartNina Anne ParacadОценок пока нет
- 2015A&PIntro CardiovascularHandoutДокумент16 страниц2015A&PIntro CardiovascularHandoutMaggieHameedОценок пока нет
- NPTE CArdio NotesДокумент27 страницNPTE CArdio NotesAubrey Vale SagunОценок пока нет
- Circulation NotesДокумент2 страницыCirculation NotesBhkti MittalОценок пока нет
- Cardiac CycleДокумент3 страницыCardiac CycleKhadijah HabeebahОценок пока нет
- Module Cardiovascular System Anatomy and PhysiologyДокумент9 страницModule Cardiovascular System Anatomy and PhysiologyPATRICIA KAYE RIOОценок пока нет
- CardiovascularДокумент6 страницCardiovascularMabes100% (1)
- Canine Heart PhysiologyДокумент52 страницыCanine Heart PhysiologyShubham HarishОценок пока нет
- Lecture Notes on Anatomy and Physiology of the Cardiovascular SystemДокумент18 страницLecture Notes on Anatomy and Physiology of the Cardiovascular SystemLudwigJayBarayuga100% (5)
- Overview of Anatomy & Physiology Assessment of CV Function: Cardiovascular SystemДокумент60 страницOverview of Anatomy & Physiology Assessment of CV Function: Cardiovascular SystemSaputra Tri NopiantoОценок пока нет
- Cardiovascular Anatomy and PhysiologyДокумент28 страницCardiovascular Anatomy and PhysiologyKris Adrian MallillinОценок пока нет
- Cardiovascular SystemДокумент14 страницCardiovascular SystemAthena Huynh100% (1)
- Cardiogenic ShockДокумент14 страницCardiogenic ShockZellanien hdОценок пока нет
- Cardiac Cycle CardiodynamicsДокумент29 страницCardiac Cycle Cardiodynamicseverforyou2023Оценок пока нет
- Cardiovascular SystemДокумент8 страницCardiovascular Systemomar farooqОценок пока нет
- Cardiovascular Physical TherapyДокумент204 страницыCardiovascular Physical Therapydivyam2008Оценок пока нет
- Circulatory Response To ExerciseДокумент31 страницаCirculatory Response To ExerciseFarhad GulОценок пока нет
- Cardiovascular System: Claire R. Hatton, RN, MANДокумент63 страницыCardiovascular System: Claire R. Hatton, RN, MANrhimineecat71Оценок пока нет
- Cardiovascular Physiology: The Autonomic Nervous SystemДокумент8 страницCardiovascular Physiology: The Autonomic Nervous SystemRidha Surya NugrahaОценок пока нет
- Cardiovascular Oral Examination ReviewДокумент6 страницCardiovascular Oral Examination ReviewJewel BerbanoОценок пока нет
- Cardiovascular System BSN 1Документ16 страницCardiovascular System BSN 1Arianne Jen GenotivaОценок пока нет
- Chapter 5 Care of The Clients With Cardiovascular DisordersДокумент226 страницChapter 5 Care of The Clients With Cardiovascular DisordersDon Felicisimo EbronОценок пока нет
- Cardiovascular Physiology: Cardiac Muscle, Rhythm, Cycle & OutputДокумент26 страницCardiovascular Physiology: Cardiac Muscle, Rhythm, Cycle & OutputPhai KoemhienОценок пока нет
- Cardionursing 110207023802 Phpapp01Документ18 страницCardionursing 110207023802 Phpapp01arvinnnnОценок пока нет
- w2 Part 1Документ30 страницw2 Part 1farahafiqahОценок пока нет
- Heart and Neck Vessels AssessmentДокумент4 страницыHeart and Neck Vessels AssessmentAndrei PedrajetaОценок пока нет
- The Heart PDFДокумент13 страницThe Heart PDFMary Ann SacramentoОценок пока нет
- Med Surg 2Документ76 страницMed Surg 2sham gowliОценок пока нет
- Riya Arya - 21msc1279 - Biology For ChemistsДокумент13 страницRiya Arya - 21msc1279 - Biology For ChemistsSwadesh SenОценок пока нет
- Acute Myocardial InfarctionДокумент62 страницыAcute Myocardial InfarctionJohn Alvin YoroОценок пока нет
- EcgДокумент2 страницыEcgR-Zee GaminGОценок пока нет
- Anatomy & Physiology Training OverviewДокумент50 страницAnatomy & Physiology Training OverviewAlisa BrownОценок пока нет
- Cardiac Anatomy and Physiology: Iris Ken R. Rico, OTRPДокумент90 страницCardiac Anatomy and Physiology: Iris Ken R. Rico, OTRPAndra HijratulОценок пока нет
- First Question: Student's Name: Adel Sulaiman SectionДокумент5 страницFirst Question: Student's Name: Adel Sulaiman SectionDental LecturesMMQОценок пока нет
- A. Cardiac Cycle: 1. Atrial Systole (Contraction of Atria) - 0.1sДокумент6 страницA. Cardiac Cycle: 1. Atrial Systole (Contraction of Atria) - 0.1sjasper haiОценок пока нет
- Chapter 20 - Introduction To The Cardiovascular System: Away From To BetweenДокумент6 страницChapter 20 - Introduction To The Cardiovascular System: Away From To Betweentomorrow.today.yesterday .yesterdayОценок пока нет
- Cardiovascular System ExplainedДокумент15 страницCardiovascular System ExplainedArif WahyuОценок пока нет
- Cardiovascular System OverviewДокумент51 страницаCardiovascular System OverviewFung Shan CheungОценок пока нет
- Cardio SlidesДокумент309 страницCardio SlidesGina VasquezОценок пока нет
- Cardiovascular SystemДокумент10 страницCardiovascular Systemsurviving nursing school100% (2)
- ECG and HEART SOUNDS EXPERIMENTДокумент10 страницECG and HEART SOUNDS EXPERIMENTMatthewFlecknoeОценок пока нет
- HeartДокумент36 страницHeartSoovendran VaradarajanОценок пока нет
- Cardiac AssessmentДокумент54 страницыCardiac AssessmentAthira PSОценок пока нет
- Circulatory SystemДокумент12 страницCirculatory System46bwilsonОценок пока нет
- Right Ventricular Myocardial InfarctionДокумент43 страницыRight Ventricular Myocardial Infarctionrudresh m g0% (2)
- Cambridge Checkpoint Science Workbook 2 AnswersДокумент33 страницыCambridge Checkpoint Science Workbook 2 AnswersmarryОценок пока нет
- Mark Scheme (Results) October 2019Документ24 страницыMark Scheme (Results) October 2019sammam mahdi samiОценок пока нет
- B F C C 18: ODY Luids AND IrculationДокумент12 страницB F C C 18: ODY Luids AND Irculation07 mathsОценок пока нет
- By: Darryl Jamison Macon County EMS Training CoordinatorДокумент53 страницыBy: Darryl Jamison Macon County EMS Training Coordinatorsharin143Оценок пока нет
- CVS/ The Blood Vessels: by DR - Ahmed Avdel MandaniДокумент27 страницCVS/ The Blood Vessels: by DR - Ahmed Avdel MandaniSerwan J AbdulrahmanОценок пока нет
- Cardiovascular SystemДокумент34 страницыCardiovascular Systemurooj100% (1)
- Unit 4 (7) Origin and Conduction of Cardiac ImpulsesДокумент31 страницаUnit 4 (7) Origin and Conduction of Cardiac ImpulsesDINAMANI 0inamОценок пока нет
- Cicrulatory and Immune Workbook KEYДокумент32 страницыCicrulatory and Immune Workbook KEYgeorgia robinsonОценок пока нет
- Pediatric and Neonatal Respiratory Care DevelopmentДокумент205 страницPediatric and Neonatal Respiratory Care DevelopmentAlexander Santiago ParelОценок пока нет
- Gross Anatomy II Lecture on Heart and Vascular SystemДокумент13 страницGross Anatomy II Lecture on Heart and Vascular SystemSantosh Bhandari100% (2)
- Defect de sept atrial etiologie embriologie patogenieДокумент4 страницыDefect de sept atrial etiologie embriologie patogenie22194Оценок пока нет
- Transport in Humans: 8.1 The Human Transport SystemДокумент11 страницTransport in Humans: 8.1 The Human Transport SystemPhylliscccОценок пока нет
- Cardiovascular System DevelopmentДокумент63 страницыCardiovascular System DevelopmentAdan Iman100% (1)
- Teorias de La ContraccionДокумент24 страницыTeorias de La ContraccionCarlos Navarro alonsoОценок пока нет
- CirculatorySystem GizmoДокумент4 страницыCirculatorySystem GizmoNashly Ramirez50% (2)
- Horse Anatomy (VetBooks - Ir)Документ36 страницHorse Anatomy (VetBooks - Ir)Ana RosaОценок пока нет
- Lecure-6 The Heat & Electrocardiogram (ECG)Документ72 страницыLecure-6 The Heat & Electrocardiogram (ECG)Noor AhmedОценок пока нет
- Pacemaker and TypesДокумент7 страницPacemaker and TypesPrathamesh ShindeОценок пока нет
- Atrial Septal DefectДокумент7 страницAtrial Septal DefectRis Amy AyaОценок пока нет
- Compare and Contrast Process in Plants and AnimalsДокумент8 страницCompare and Contrast Process in Plants and AnimalsKimberly EamilaoОценок пока нет
- ECG Mastery Improving Your ECG Interpretation SkillsДокумент23 страницыECG Mastery Improving Your ECG Interpretation SkillsHitesh Deora100% (2)
- Mitral Regurgitation: Jacqueline Suk Danik,, and Bernard E. BulwerДокумент30 страницMitral Regurgitation: Jacqueline Suk Danik,, and Bernard E. Bulwerhawk.man8Оценок пока нет
- Test - Embryology Practice Questions With Answers - QuizletДокумент10 страницTest - Embryology Practice Questions With Answers - QuizletAziz100% (1)
- Circulatory System GlossaryДокумент2 страницыCirculatory System Glossarykloaizar100% (1)
- Chapter08 PDFДокумент30 страницChapter08 PDFEnfermeriaAncamОценок пока нет
- Nclex Cheat SheetДокумент6 страницNclex Cheat SheetLeeAnn Marie100% (34)
- Fundamentals of Cardiology For The USMLE and General Medics PDFДокумент287 страницFundamentals of Cardiology For The USMLE and General Medics PDFCharles Vindo100% (2)
- Main Applications of ECG DiagnosisДокумент19 страницMain Applications of ECG DiagnosisMaria Rowena O. SalvoОценок пока нет