Вам также может понравиться
- Soap Note Week 1 Sep7Документ3 страницыSoap Note Week 1 Sep7dondavis77Оценок пока нет
- Dermatitis SOAP NOTEДокумент10 страницDermatitis SOAP NOTEHugs100% (2)
- Chapter 3 SOAP NoteДокумент2 страницыChapter 3 SOAP NoteKatrina Litzko50% (2)
- Final Check Off Soap NoteДокумент4 страницыFinal Check Off Soap Notesana100% (1)
- SoapДокумент5 страницSoapallele940% (1)
- Create SOAP Notes Using Medical TerminologyДокумент4 страницыCreate SOAP Notes Using Medical TerminologyLatora Gardner Boswell100% (3)
- Headache H&P SOAPДокумент3 страницыHeadache H&P SOAPRauf Ab67% (3)
- SOAP NoteДокумент8 страницSOAP NoteAnonymous p0y5mmLQОценок пока нет
- Nsg6435 Soap Note 2Документ7 страницNsg6435 Soap Note 2Hephzibah Beulah100% (1)
- Soap Note 1Документ3 страницыSoap Note 1Heather CunninghamОценок пока нет
- Soap Note 3 FinalДокумент9 страницSoap Note 3 Finalapi-272656243Оценок пока нет
- Physical Exam ChecklistДокумент2 страницыPhysical Exam ChecklistRaisah Bint Abdullah100% (5)
- Soap Note 3 DominguezДокумент6 страницSoap Note 3 Dominguezapi-320062911Оценок пока нет
- ICM SOAP Note 11:3Документ4 страницыICM SOAP Note 11:3Warren G Lawless67% (3)
- Soap Note1 - Gyn ComplaintДокумент6 страницSoap Note1 - Gyn Complaintapi-482726932100% (3)
- Soap 1Документ7 страницSoap 1api-248360288Оценок пока нет
- Primary Care Case: Sore ThroatДокумент9 страницPrimary Care Case: Sore Throatarunateja100% (2)
- Soap NotesДокумент1 страницаSoap Notesjcfx2100% (1)
- Final Practicum - Soap Note 3Документ17 страницFinal Practicum - Soap Note 3api-494643478100% (2)
- Chronic SOAP Note for 51 Year Old Female with HyperlipidemiaДокумент3 страницыChronic SOAP Note for 51 Year Old Female with HyperlipidemiaJeffrey ViernesОценок пока нет
- Red eye with dischargeДокумент4 страницыRed eye with dischargeเด็กชายท็อปปิ้ง ชอบกลิ้งเข้าคณะเภสัชศาสตร์Оценок пока нет
- SOAP Note Cheat Sheet - Complete H&PДокумент2 страницыSOAP Note Cheat Sheet - Complete H&PAdeline N. Omene95% (19)
- SOAP Sample 1Документ6 страницSOAP Sample 1AyeshaArif100% (1)
- Soap Note 2 Dominguez 2015Документ5 страницSoap Note 2 Dominguez 2015api-320062911Оценок пока нет
- Peds - Soap Note 5Документ3 страницыPeds - Soap Note 5api-546259691Оценок пока нет
- NU 665 Pediatric Gastrointestinal Case Study - Michelle - StewardДокумент10 страницNU 665 Pediatric Gastrointestinal Case Study - Michelle - StewardMichelle StewardОценок пока нет
- Sample Soap NoteДокумент12 страницSample Soap NoteSedaka Donaldson0% (1)
- Nurs 5018 - Soap Note Chronic IllnessДокумент5 страницNurs 5018 - Soap Note Chronic Illnessapi-308904543Оценок пока нет
- SOAP NoteДокумент3 страницыSOAP NoteMagdala D'autruche100% (1)
- Focused Soap NoteДокумент4 страницыFocused Soap Noteapi-24735887592% (13)
- Adult Health - Soap Note 5Документ3 страницыAdult Health - Soap Note 5api-546259691100% (3)
- SOAP 2 - KhanДокумент11 страницSOAP 2 - KhanMohammad KhanОценок пока нет
- Soap Note - Musculoskeletal and Nervous SystemsДокумент2 страницыSoap Note - Musculoskeletal and Nervous SystemsSummer Keller88% (8)
- Danny Rivera SOAPДокумент4 страницыDanny Rivera SOAPariel sparkman100% (1)
- Contraception SOAP Note ReviewДокумент7 страницContraception SOAP Note ReviewAnnah AnnОценок пока нет
- Abdominal Pain Diagnosis and Treatment PlanДокумент2 страницыAbdominal Pain Diagnosis and Treatment PlanSandhya Rubens67% (9)
- Soap NotesДокумент2 страницыSoap Notesapi-380833341100% (1)
- 11 - Dot Phrase Templates HMC ED June 2017 - Rev 9.6.17Документ13 страниц11 - Dot Phrase Templates HMC ED June 2017 - Rev 9.6.17M100% (1)
- SOAP Annual PhysicalДокумент11 страницSOAP Annual Physicalniknshell100% (1)
- H&P For ScriptДокумент12 страницH&P For ScriptAlina KievskyОценок пока нет
- Nurs 5023 - Soap 5Документ5 страницNurs 5023 - Soap 5api-308904543100% (2)
- Nursing NoteДокумент6 страницNursing Noteshiller0% (1)
- Sample Soap NoteДокумент7 страницSample Soap Notesedaka260% (1)
- Soap NoteДокумент4 страницыSoap Noteapi-252633788100% (7)
- Acute Cholecystitis ER AdmissionДокумент6 страницAcute Cholecystitis ER Admissionjessica100% (5)
- Soap Well Women S KellyДокумент6 страницSoap Well Women S Kellyapi-415083061Оценок пока нет
- Adult - Case StudyДокумент14 страницAdult - Case Studyapi-494643478100% (2)
- SOAP Note AdviceДокумент5 страницSOAP Note AdviceNico AvellanaОценок пока нет
- Patient History and Presentation SkillsДокумент4 страницыPatient History and Presentation Skillsbnarnold100% (2)
- Peds 4 Soap Note S Kelly 5023 100 From KellyДокумент12 страницPeds 4 Soap Note S Kelly 5023 100 From Kellyapi-415083061Оценок пока нет
- SOAP For Upper Respiratory Infection #4Документ3 страницыSOAP For Upper Respiratory Infection #4carlos fernandezОценок пока нет
- Soap 5 - Geriatric 65Документ13 страницSoap 5 - Geriatric 65api-482726932Оценок пока нет
- Esther Park - SOAP NOTE - Abdominal PainДокумент4 страницыEsther Park - SOAP NOTE - Abdominal PainMallory ZaborОценок пока нет
- TB Soap NoteДокумент1 страницаTB Soap NoteNumerator0% (1)
- Textbook of Urgent Care Management: Chapter 17, Physician Extenders in the Urgent Care CenterОт EverandTextbook of Urgent Care Management: Chapter 17, Physician Extenders in the Urgent Care CenterОценок пока нет
- The Nurse Practitioner in UrologyОт EverandThe Nurse Practitioner in UrologyMichelle LajinessОценок пока нет
- Back to Zero: FNP Board Review NotesОт EverandBack to Zero: FNP Board Review NotesРейтинг: 5 из 5 звезд5/5 (2)
- FAMILY NURSE PRACTITIONER: Passbooks Study GuideОт EverandFAMILY NURSE PRACTITIONER: Passbooks Study GuideОценок пока нет
- Herbal Antibiotics: A Review: October 2020Документ8 страницHerbal Antibiotics: A Review: October 2020srikanth PosaОценок пока нет
- Psychiatry MCQ-Answer-Book PDFДокумент12 страницPsychiatry MCQ-Answer-Book PDFWorku Kifle100% (2)
- GBTPP PHKДокумент59 страницGBTPP PHKSyahrul Tuba Al FatihОценок пока нет
- 04-05-2020 - Non Compartment AnalysisДокумент3 страницы04-05-2020 - Non Compartment AnalysisTHE SMURFSОценок пока нет
- Ayahuasca 2022Документ17 страницAyahuasca 2022Doctor LeoОценок пока нет
- Hemodynamic Management Pocket Card PDFДокумент8 страницHemodynamic Management Pocket Card PDFjenn1722Оценок пока нет
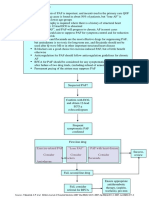
- Pathway DIAGNOSIS OF PAF FTRДокумент1 страницаPathway DIAGNOSIS OF PAF FTRYoan Eka Putra PalilingОценок пока нет
- The Neurobiology of AutismДокумент15 страницThe Neurobiology of AutismArif KurniawanОценок пока нет
- DM Type 2Документ9 страницDM Type 2Gates FebriОценок пока нет
- Naloxone HydrochlorideДокумент3 страницыNaloxone HydrochlorideDanish MaqboolОценок пока нет
- Solved Suppose That in The Repeated Bertrand Model Discussed in SectionДокумент1 страницаSolved Suppose That in The Repeated Bertrand Model Discussed in SectionM Bilal SaleemОценок пока нет
- Article WJPR 1513745964Документ12 страницArticle WJPR 1513745964Sivakumar LakshminarayananОценок пока нет
- A Milestone in Codifying The Wisdom of Traditional Oriental Medicine: TCM, Kampo, TKM, TVM-WHO International Standard Terminologies On Traditional Medicine in The Western Pacific RegionДокумент3 страницыA Milestone in Codifying The Wisdom of Traditional Oriental Medicine: TCM, Kampo, TKM, TVM-WHO International Standard Terminologies On Traditional Medicine in The Western Pacific RegionDimas RfОценок пока нет
- Pcol Cover To CoverДокумент214 страницPcol Cover To CoverJec OcampoОценок пока нет
- 85beb4c0-49be-4351-b700-ee2fc36a7ab6Документ90 страниц85beb4c0-49be-4351-b700-ee2fc36a7ab6imgamer.msОценок пока нет
- Zinc Oxide USP 31Документ5 страницZinc Oxide USP 31Gracelyn GatusОценок пока нет
- Validate Cleaning Method for Flunixin Meglumine ResidueДокумент14 страницValidate Cleaning Method for Flunixin Meglumine ResiduePatricia Joyce Malabanan SunglaoОценок пока нет
- Chapter 1 Dispensing Labelling MeДокумент10 страницChapter 1 Dispensing Labelling MeQasim Jalali NanotiОценок пока нет
- Drug Metabolism - Phase IIДокумент26 страницDrug Metabolism - Phase IIalexpharmОценок пока нет
- Chewing Guava L-WPS Office YasДокумент5 страницChewing Guava L-WPS Office Yasmady everardОценок пока нет
- Character, Onset, Location, Duration, Severity, Pattern and Associated - FactorsДокумент1 страницаCharacter, Onset, Location, Duration, Severity, Pattern and Associated - FactorsJohn CuencoОценок пока нет
- NYSTATIN-nys Tatin S Us Pens Ion Morton Grove Pharmaceuticals, IncДокумент5 страницNYSTATIN-nys Tatin S Us Pens Ion Morton Grove Pharmaceuticals, IncZeyad A AbdullahОценок пока нет
- Post-Stroke Depression - A ReviewДокумент20 страницPost-Stroke Depression - A Reviewkenth nathanОценок пока нет
- Workshop 8. Badac Plan of ActionДокумент1 страницаWorkshop 8. Badac Plan of Actionjudy mar delacruzОценок пока нет
- Transdermal Drug Delivery System ReviewДокумент8 страницTransdermal Drug Delivery System ReviewParth SahniОценок пока нет
- Malarone JuniorДокумент5 страницMalarone Juniorhannah.g.pavОценок пока нет
- A Drug Study On EpinephrineДокумент7 страницA Drug Study On EpinephrineMaesy Garcia LorenaОценок пока нет
- Mehlmanmedical Hy Neuro Part IДокумент18 страницMehlmanmedical Hy Neuro Part IAzlan OmarОценок пока нет
- Anesthesia in Dentistry and Extraction of Tooth by Pratyasha ParipurnaДокумент42 страницыAnesthesia in Dentistry and Extraction of Tooth by Pratyasha ParipurnapariОценок пока нет
- Basetext SingleДокумент129 страницBasetext SingleJiHyun ParkОценок пока нет