Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- In-Service Welding of Pipelines Industry Action PlanДокумент13 страницIn-Service Welding of Pipelines Industry Action Planعزت عبد المنعم100% (1)
- BS746 2014Документ22 страницыBS746 2014marco SimonelliОценок пока нет
- Chapter Three: 1 - The Coarse Grain SoilsДокумент21 страницаChapter Three: 1 - The Coarse Grain SoilsSalih MohayaddinОценок пока нет
- Natural Disasters Vocabulary Exercises Fun Activities Games Icebreakers Oneonone Activiti 42747Документ2 страницыNatural Disasters Vocabulary Exercises Fun Activities Games Icebreakers Oneonone Activiti 42747Andrea Tercero VillarroelОценок пока нет
- Math 202 Syllabus-Spring18 PDFДокумент2 страницыMath 202 Syllabus-Spring18 PDFvonacoc49Оценок пока нет
- Ge Fairchild Brochure PDFДокумент2 страницыGe Fairchild Brochure PDFDharmesh patelОценок пока нет
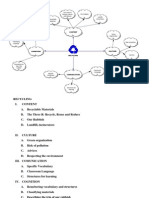
- Recycling Mind MapДокумент2 страницыRecycling Mind Mapmsole124100% (1)
- Smoldering Combustion: Guillermo ReinДокумент20 страницSmoldering Combustion: Guillermo ReinAhmed HussainОценок пока нет
- Bahir Dar University BIT: Faculity of Mechanical and Industrial EngineeringДокумент13 страницBahir Dar University BIT: Faculity of Mechanical and Industrial Engineeringfraol girmaОценок пока нет
- Comparison of 3 Tests To Detect Acaricide ResistanДокумент4 страницыComparison of 3 Tests To Detect Acaricide ResistanMarvelous SungiraiОценок пока нет
- Propert 447-445Документ11 страницPropert 447-445LUNA100% (1)
- Fama Fraternitatis Rosae Crucis PDFДокумент2 страницыFama Fraternitatis Rosae Crucis PDFJudy50% (2)
- Kwasaki ZX10R 16Документ101 страницаKwasaki ZX10R 16OliverОценок пока нет
- L GH Catalog PullingДокумент60 страницL GH Catalog PullingLuis LuperdiОценок пока нет
- Vallarpadam Terminal ChallengesДокумент3 страницыVallarpadam Terminal Challengespriya rajeev100% (1)
- Product Lifecycle Management and Sustainable Development in The Context of Industry 4.0: A Systematic Literature ReviewДокумент10 страницProduct Lifecycle Management and Sustainable Development in The Context of Industry 4.0: A Systematic Literature ReviewJosip StjepandicОценок пока нет
- Assignment 4 SolutionsДокумент9 страницAssignment 4 SolutionsNengke Lin100% (2)
- DCS YokogawaДокумент17 страницDCS Yokogawasswahyudi100% (1)
- Final TestДокумент10 страницFinal TestbennyОценок пока нет
- Solid Modeling Techniques: Constructive Solid Geometry (CSG)Документ22 страницыSolid Modeling Techniques: Constructive Solid Geometry (CSG)amolОценок пока нет
- Germania Agenturinfo enДокумент4 страницыGermania Agenturinfo enДушан СтепановићОценок пока нет
- Chapter 1 (PLC)Документ9 страницChapter 1 (PLC)Kibria PrangonОценок пока нет
- #Dr. Lora Ecg PDFДокумент53 страницы#Dr. Lora Ecg PDFمحمد زينОценок пока нет
- All About PlantsДокумент14 страницAll About Plantsapi-234860390Оценок пока нет
- Engineering Structures: C.X. Dong, A.K.H. Kwan, J.C.M. HoДокумент14 страницEngineering Structures: C.X. Dong, A.K.H. Kwan, J.C.M. HoElieser SinagaОценок пока нет
- Eliminating Oscillation Between Parallel MnosfetsДокумент6 страницEliminating Oscillation Between Parallel MnosfetsCiprian BirisОценок пока нет
- St. John's Wort: Clinical OverviewДокумент14 страницSt. John's Wort: Clinical OverviewTrismegisteОценок пока нет
- Raspberry Pi 3 and BeagleBone Black For Engineers - UpSkill Learning 124Документ124 страницыRaspberry Pi 3 and BeagleBone Black For Engineers - UpSkill Learning 124Dragan IvanovОценок пока нет
- Generative Shape DesignДокумент195 страницGenerative Shape DesignAdi Fiera100% (1)