Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- MCQs Chapter Test 9Документ4 страницыMCQs Chapter Test 9wjeelani100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- NA To Sls en 1993-1-4Документ12 страницNA To Sls en 1993-1-4Shan Sandaruwan AbeywardeneОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Railways Industry: To Increase Your Productivity, Optimize Maintenance and Repair With Long-Life Filler MetalsДокумент2 страницыRailways Industry: To Increase Your Productivity, Optimize Maintenance and Repair With Long-Life Filler Metalskamals55Оценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
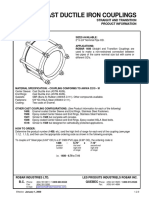
- P Robar 1408 Cast Ductile Iron CouplingsДокумент1 страницаP Robar 1408 Cast Ductile Iron CouplingsBrandon HoltenОценок пока нет
- PDF Interpolacion Polinomica de Lagrange CompressДокумент41 страницаPDF Interpolacion Polinomica de Lagrange CompressJuan Sebastián Romero DíazОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- JIS G3106 SM490YB: Welded Structure Steel PlateДокумент1 страницаJIS G3106 SM490YB: Welded Structure Steel PlateTh NattapongОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- A 3 14 PDFДокумент272 страницыA 3 14 PDFRahardian Faizal ZuhdiОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Sand Casting Over View and Defect AnalysisДокумент29 страницSand Casting Over View and Defect AnalysisNindya HauraОценок пока нет
- Tablas Metalurgicas 1-2 PDFДокумент4 страницыTablas Metalurgicas 1-2 PDFAnonymous CNormeuqWpОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- S 700Документ12 страницS 700HeiderHuertaОценок пока нет
- Maithan AlloysДокумент16 страницMaithan AlloysVanshajОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Precision Aerospace FastenersДокумент4 страницыPrecision Aerospace FastenersАндрей МошкинОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Zero Defect Strategy Download 17-11-09Документ9 страницZero Defect Strategy Download 17-11-09Jagadeesh NandamОценок пока нет
- BOM-Alfa Co2 Welding Fixture - HardwareДокумент9 страницBOM-Alfa Co2 Welding Fixture - HardwareBhavesh ShiyaniОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Effects of Icosahedral Phase Formation On The Microstructure and Mechanical Improvement of MG Alloys: A ReviewДокумент22 страницыEffects of Icosahedral Phase Formation On The Microstructure and Mechanical Improvement of MG Alloys: A Reviewshouxun JiОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Steel - Continuous CastingДокумент11 страницSteel - Continuous CastingAli AzharОценок пока нет
- 09 Wood Chisels PlanesДокумент7 страниц09 Wood Chisels PlanesPriОценок пока нет
- DFM & Dfa 302Документ37 страницDFM & Dfa 302YASH BHAVSARОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Condenser Tube Failure GeneralДокумент273 страницыCondenser Tube Failure GeneralRagvendra BistОценок пока нет
- Iron and SteelДокумент21 страницаIron and SteelananthaaОценок пока нет
- TDS NORD TEST U 88 EnglishДокумент4 страницыTDS NORD TEST U 88 EnglishnОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Steel Mill Industrial TrainingДокумент34 страницыSteel Mill Industrial TrainingBenОценок пока нет
- General Hss End Mills Yg1Документ60 страницGeneral Hss End Mills Yg1bayuwiroОценок пока нет
- Middle Ear Implants Reference GuideДокумент15 страницMiddle Ear Implants Reference GuideChaovarin PattarachokchuyОценок пока нет
- SB 677Документ6 страницSB 677FrengkiОценок пока нет
- API 570 Exam Publications Effectivity Sheet: June 2021 and October 2021Документ1 страницаAPI 570 Exam Publications Effectivity Sheet: June 2021 and October 2021pmkarОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- IS 4049-2 (1996) Formed Ends For Tanks and Pressure (Inside Diameter Basis) PDFДокумент14 страницIS 4049-2 (1996) Formed Ends For Tanks and Pressure (Inside Diameter Basis) PDFShivprasadОценок пока нет
- AWWA D100-11 PreДокумент6 страницAWWA D100-11 PremojeebmashalОценок пока нет
- The Welding Handbook For Maritime WeldersДокумент552 страницыThe Welding Handbook For Maritime WeldersStefanus Pradika Widcaksono100% (1)